

OVERVIEW OF UPPER LIMB
COMPARISON OF UPPER AND LOWER LIMBS
BONES OF UPPER LIMB
Clavicle
Scapula
Humerus
Bones of Forearm
Bones of Hand
Surface Anatomy of Upper Limb Bones
BLUE BOX: Bones of Upper Limb. Upper Limb Injuries; Variations of Clavicle; Fracture of Clavicle; Ossification of Clavicle; Fracture of Scapula; Fractures of Humerus; Fractures of Radius and Ulna; Fracture of Scaphoid; Fracture of Hamate; Fracture of Metacarpals; Fracture of Phalanges
FASCIA, EFFERENT VESSELS, CUTANEOUS INNERVATION, AND MYOTOMES OF UPPER LIMB
Fascia of Upper Limb
Venous Drainage of Upper Limb
Lymphatic Drainage of Upper Limb
Cutaneous Innervation of Upper Limb
Motor Innervation (Myotomes) of Upper Limb
TABLE 6.1. Dermatomes of Upper Limb
TABLE 6.2. Cutaneous Nerves of Upper Limb
PECTORAL AND SCAPULAR REGIONS
Anterior Axio-appendicular Muscles
TABLE 6.3. Anterior Axio-appendicular Muscles
Posterior Axio-appendicular and Scapulohumeral Muscles
TABLE 6.4. Posterior Axio-appendicular Muscles
TABLE 6.5. Movements of Scapula
Scapulohumeral (Intrinsic Shoulder) Muscles
TABLE 6.6. Scapulohumeral (Intrinsic Shoulder) Muscles
Surface Anatomy of Pectoral, Scapular, and Deltoid Regions
BLUE BOX: Pectoral, Scapular, and Deltoid Regions. Absence of Pectoral Muscles; Paralysis of Serratus Anterior; Triangle of Auscultation; Injury of Spinal Accessory Nerve (CN XI); Injury of Thoracodorsal Nerve; Injury to Dorsal Scapular Nerve; Injury to Axillary Nerve; Fracture–Dislocation of Proximal Humeral Epiphysis; Rotator Cuff Injuries
AXILLA
Axillary Artery
TABLE 6.7. Arteries of Proximal Upper Limb (Shoulder Region and Arm)
Axillary Vein
Axillary Lymph Nodes
Brachial Plexus
TABLE 6.8. Brachial Plexus and Nerves of Upper Limb
BLUE BOX: Axilla. Arterial Anastomoses Around Scapula; Compression of Axillary Artery; Aneurysm of Axillary Artery; Injuries to Axillary Vein; Role of Axillary Vein in Subclavian Vein Puncture; Enlargement of Axillary Lymph Nodes; Dissection of Axillary Lymph Nodes; Variations of Brachial Plexus; Brachial Plexus Injuries; Brachial Plexus Block
ARM
Muscles of Arm
TABLE 6.9. Muscles of Arm
Brachial Artery
Veins of Arm
Nerves of Arm
Cubital Fossa
Surface Anatomy of Arm and Cubital Fossa
BLUE BOX: Arm and Cubital Fossa. Bicipital Myotatic Reflex; Biceps Tendinitis; Dislocation of Tendon of Long Head of Biceps Brachii; Rupture of Tendon of Long Head of Biceps Brachii; Interruption of Blood Flow in Brachial Artery; Fracture of Humeral Shaft; Injury to Musculocutaneous Nerve; Injury to Radial Nerve in Arm; Venipuncture in Cubital Fossa; Variation of Veins in Cubital Fossa
FOREARM
Compartments of Forearm
Muscles of Forearm
TABLE 6.10. Muscles of Anterior Compartment of Forearm
TABLE 6.11. Muscles of Posterior Compartment of Forearm
Arteries of Forearm
TABLE 6.12. Arteries of Forearm and Wrist
Veins of Forearm
Nerves of Forearm
TABLE 6.13. Nerves of Forearm
Surface Anatomy of Forearm
BLUE BOX: Forearm. Elbow Tendinitis or Lateral Epicondylitis; Mallet or Baseball Finger; Fracture of Olecranon; Synovial Cyst of Wrist; High Division of Brachial Artery; Superficial Ulnar Artery; Measuring Pulse Rate; Variations in Origin of Radial Artery; Median Nerve Injury; Pronator Syndrome; Communications Between Median and Ulnar Nerves; Injury of Ulnar Nerve at Elbow and in Forearm; Cubital Tunnel Syndrome; Injury of Radial Nerve in Forearm (Superficial or Deep Branches)
HAND
Fascia and Compartments of Palm
Muscles of Hand
TABLE 6.14. Intrinsic Muscles of Hand
Long Flexor Tendons and Tendon Sheaths in Hand
Arteries of Hand
TABLE 6.15. Arteries of Hand
Veins of Hand
Nerves of Hand
TABLE 6.16. Nerves of Hand
Surface Anatomy of Hand
BLUE BOX: Hand. Dupuytren Contracture of Palmar Fascia; Hand Infections; Tenosynovitis; Laceration of Palmar Arches; Ischemia of Digits (Fingers); Lesions of Median Nerve; Carpal Tunnel Syndrome; Trauma to Median Nerve; Ulnar Canal Syndrome; Handlebar Neuropathy; Radial Nerve Injury in Arm and Hand Disability; Dermatoglyphics; Palmar Wounds and Surgical Incisions
Joints of Upper Limb
Sternoclavicular Joint
Acromioclavicular Joint
Glenohumeral Joint
Elbow Joint
TABLE 6.17. Movements of Glenohumeral Joint
Proximal Radio-Ulnar Joint
Distal Radio-Ulnar Joint
Wrist Joint
Intercarpal Joints
Carpometacarpal and Intermetacarpal Joints
Metacarpophalangeal and Interphalangeal Joints
BLUE BOX: Joints of Upper Limb. Dislocation of Sternoclavicular Joint; Ankylosis of Sternoclavicular Joint; Dislocation of Acromioclavicular Joint; Calcific Supraspinatus Tendinitis; Rotator Cuff Injuries; Dislocation of Glenohumeral Joint; Axillary Nerve Injury; Glenoid Labrum Tears; Adhesive Capsulitis of Glenohumeral Joint; Bursitis of Elbow; Avulsion of Medial Epicondyle; Ulnar Collateral Ligament Reconstruction; Dislocation of Elbow Joint; Subluxation and Dislocation of Radial Head; Wrist Fractures and Dislocations; Bull Rider’s Thumb; Skier’s Thumb
OVERVIEW OF UPPER LIMB
The upper limb is characterized by its mobility and ability to grasp, strike, and conduct fine motor skills (manipulation). These characteristics are especially marked in the hand when performing manual activities, such as buttoning a shirt.
Synchronized interplay occurs between the joints of the upper limb to coordinate the intervening segments to perform smooth, efficient motion at the most workable distance or position required for a specific task. Efficiency of hand function results in large part from the ability to place it in the proper position by movements at the scapulothoracic, glenohumeral, elbow, radio-ulnar, and wrist joints.
The upper limb consists of four major segments, which are further subdivided into regions for precise description (Figs. 6.1 and 6.2):
1. Shoulder: proximal segment of the limb that overlaps parts of the trunk (thorax and back) and lower lateral neck. It includes the pectoral, scapular, and deltoid regions of the upper limb, and the lateral part (greater supraclavicular fossa) of the lateral cervical region. It overlies half of the pectoral girdle. The pectoral girdle (shoulder girdle) is a bony ring, incomplete posteriorly, formed by the scapulae and clavicles, and completed anteriorly by the manubrium of the sternum (part of the axial skeleton).
2. Arm (L. brachium): first segment of the free upper limb (more mobile part of the upper limb independent of the trunk) and the longest segment of the limb. It extends between and connects the shoulder and the elbow, and consists of anterior and posterior regions of the arm, centered around the humerus.
3. Forearm (L. antebrachium): second longest segment of the limb. It extends between and connects the elbow and wrist and includes anterior and posterior regions of the forearm overlying the radius and ulna.
4. Hand (L. manus): part of the upper limb distal to the forearm that is formed around the carpus, metacarpus, and phalanges. It is composed of the wrist, palm, dorsum of hand, and digits (fingers, including an opposable thumb), and is richly supplied with sensory endings for touch, pain, and temperature.

FIGURE 6.1. Segments and bones of upper limb. The joints divide the superior appendicular skeleton, and thus the limb itself, into four main segments: shoulder, arm, forearm, and hand.

FIGURE 6.2. Regions of upper limb. For exact description, the upper limb is divided into regions based on the external features (surface anatomy) of the underlying muscular formations, bones, and joints.
COMPARISON OF UPPER AND LOWER LIMBS
Developing in a similar fashion, the upper and lower limbs share many common features (see Chapter 5). However, they are sufficiently distinct in structure to enable markedly different functions and abilities. Because the upper limb is not usually involved in weight bearing or motility, its stability has been sacrificed to gain mobility. The upper limb still possesses remarkable strength; and because of the hand’s ability to conform to a paddle or assume a gripping or platform configuration, it may assume a role in motility in certain circumstances.
Both the upper and the lower limbs are connected to the axial skeleton (cranium, vertebral column, and associated thoracic cage) via the bony pectoral and pelvic girdles, respectively. The pelvic girdle consists of the two hip bones connected to the sacrum (see Chapter 5). The pectoral girdle consists of the scapulae and clavicles, connected to the manubrium of the sternum. Both girdles possess a large flat bone located posteriorly, which provides for attachment of proximal muscles, and connects with its contralateral partner anteriorly via small bony braces, the pubic rami and clavicles. However, the flat iliac bones of the pelvic girdle are also connected posteriorly through their primary attachment to the sacrum via the essentially rigid, weight-transferring sacro-iliac joints. This posterior connection to the axial skeleton places the lower limbs inferior to the trunk, enabling them to be supportive as they function primarily in relation to the line of gravity. Furthermore, because the two sides are connected both anteriorly and posteriorly, the pelvic girdle forms a complete rigid ring that limits mobility, making the movements of one limb markedly affect the movements of the other. The pectoral girdle, however, is connected to the trunk only anteriorly, via the sternum, by flexible joints with 3 degrees of freedom. It is an incomplete ring because the scapulae are not connected with each other posteriorly. Thus, the motion of one upper limb is independent of the other, and the limbs are able to operate effectively anterior to the body, at a distance and level that enable precise eye–hand coordination.
In both the upper and the lower limbs, the long bone of the most proximal segment is the largest and is unpaired. The long bones increase progressively in number but decrease in size in the more distal segments of the limb. The second most proximal segment of both limbs (i.e., the leg and forearm) has two parallel bones, although only in the forearm do both articulate with the bone of the proximal segment, and only in the leg do both articulate directly with the distal segment. Although the paired bones of both the leg and forearm flex and extend as a unit, only those of the upper limb are able to move (supinate and pronate) relative to each other; the bones of the leg are fixed in the pronated position.
The wrist and ankle have a similar number of short bones (eight and seven, respectively). Both groups of short bones interrupt a series of long bones that resumes distally with several sets of long bones of similar lengths, with a similar number of joints of essentially the same type. The digits of the upper limb (fingers including the thumb) are the most mobile parts of either limb. However, all other parts of the upper limb are more mobile than the comparable parts of the lower limb.
BONES OF UPPER LIMB
The pectoral girdle and bones of the free part of the upper limb form the superior appendicular skeleton (Fig. 6.3); the pelvic girdle and bones of the free part of the lower limb form the inferior appendicular skeleton. The superior appendicular skeleton articulates with the axial skeleton only at the sternoclavicular joint, allowing great mobility. The clavicles and scapulae of the pectoral girdle are supported, stabilized, and moved by axio-appendicular muscles that attach to the relatively fixed ribs, sternum, and vertebrae of the axial skeleton.
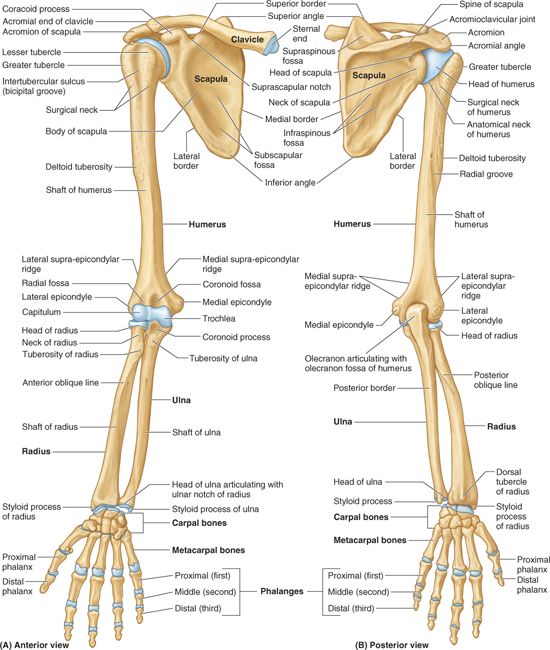
FIGURE 6.3. Bones of upper limb.
Clavicle
The clavicle (collar bone) connects the upper limb to the trunk (Figs. 6.3 and 6.4). The shaft of the clavicle has a double curve in a horizontal plane. Its medial half is convex anteriorly, and its sternal end is enlarged and triangular where it articulates with the manubrium of the sternum at the sternoclavicular (SC) joint. Its lateral half is concave anteriorly, and its acromial end is flat where it articulates with the acromion of the scapula at the acromioclavicular (AC) joint (Figs. 6.3B and 6.4). The medial two thirds of the shaft of the clavicle are convex anteriorly, whereas the lateral third is flattened and concave anteriorly. These curvatures increase the resilience of the clavicle, and give it the appearance of an elongated capital S.

FIGURE 6.4. Right clavicle. Prominent features of the superior and inferior surfaces of the clavicle. The bone acts as a mobile strut (supporting brace) connecting the upper limb to the trunk; its length allows the limb to pivot around the trunk.
The clavicle:
• Serves as a moveable, crane-like strut (rigid support) from which the scapula and free limb are suspended, keeping them away from the trunk so that the limb has maximum freedom of motion. The strut is movable and allows the scapula to move on the thoracic wall at the “scapulothoracic joint,”1 increasing the range of motion of the limb. Fixing the strut in position, especially after its elevation, enables elevation of the ribs for deep inspiration.
• Forms one of the bony boundaries of the cervico-axillary canal (passageway between the neck and arm), affording protection to the neurovascular bundle supplying the upper limb.
• Transmits shocks (traumatic impacts) from the upper limb to the axial skeleton.
Although designated as a long bone, the clavicle has no medullary (marrow) cavity. It consists of spongy (trabecular) bone with a shell of compact bone.
The superior surface of the clavicle, lying just deep to the skin and platysma (G. flat plate) muscle in the subcutaneous tissue, is smooth.
The inferior surface of the clavicle is rough because strong ligaments bind it to the 1st rib near its sternal end and suspend the scapula from its acromial end. The conoid tubercle, near the acromial end of the clavicle (Fig. 6.4), gives attachment to the conoid ligament, the medial part of the coracoclavicular ligament by which the remainder of the upper limb is passively suspended from the clavicle. Also, near the acromial end of the clavicle is the trapezoid line, to which the trapezoid ligament attaches; it is the lateral part of the coracoclavicular ligament.
The subclavian groove (groove for the subclavius) in the medial third of the shaft of the clavicle is the site of attachment of the subclavius muscle. More medially is the impression for the costoclavicular ligament, a rough, often depressed, oval area that gives attachment to the ligament binding the 1st rib (L. costa) to the clavicle, limiting elevation of the shoulder.
Scapula
The scapula (shoulder blade) is a triangular flat bone that lies on the posterolateral aspect of the thorax, overlying the 2nd–7th ribs (see Fig. I.11, p. 20). The convex posterior surface of the scapula is unevenly divided by a thick projecting ridge of bone, the spine of the scapula, into a small supraspinous fossa and a much larger infraspinous fossa (Fig. 6.5A). The concave costal surface of most of the scapula forms a large subscapular fossa. The broad bony surfaces of the three fossae provide attachments for fleshy muscles. The triangular body of the scapula is thin and translucent superior and inferior to the spine of the scapula; although its borders, especially the lateral one, are somewhat thicker. The spine continues laterally as the flat, expanded acromion (G. akros, point), which forms the subcutaneous point of the shoulder and articulates with the acromial end of the clavicle. The deltoid tubercle of the scapular spine is the prominence indicating the medial point of attachment of the deltoid. The spine and acromion serve as levers for the attached muscles, particularly the trapezius.

FIGURE 6.5. Right scapula. A. The bony features of the costal and posterior surfaces of the scapula. B. The borders and angles of the scapula. C. The scapula is suspended from the clavicle by the coracoclavicular ligament, at which a balance is achieved among the weight of the scapula and its attached muscles plus the muscular activity medially and the weight of the free limb laterally.
Because the acromion is a lateral extension of the scapula, the AC joint is placed lateral to the mass of the scapula and its attached muscles (Fig. 6.5C). The glenohumeral (shoulder) joint on which these muscles operate is almost directly inferior to the AC joint; thus the scapular mass is balanced with that of the free limb, and the suspending structure (coracoclavicular ligament) lies between the two masses.
Superolaterally, the lateral surface of the scapula has a glenoid cavity (G. socket), which receives and articulates with the head of the humerus at the glenohumeral joint (Fig. 6.5A & C). The glenoid cavity is a shallow, concave, oval fossa (L. fossa ovalis), directed anterolaterally and slightly superiorly—that is considerably smaller than the ball (head of the humerus) for which it serves as a socket. The beak-like coracoid process (G. korak-odés, like a crow’s beak) is superior to the glenoid cavity, and projects anterolaterally. This process also resembles in size, shape, and direction a bent finger pointing to the shoulder, the knuckle of which provides the inferior attachment for the passively supporting coracoclavicular ligament.
The scapula has medial, lateral, and superior borders and superior, lateral, and inferior angles (Fig. 6.5B). When the scapular body is in the anatomical position, the thin medial border of the scapula runs parallel to and approximately 5 cm lateral to the spinous processes of the thoracic vertebrae; hence it is often called the vertebral border (Fig. 6.5B). From the inferior angle, the lateral border of the scapula runs superolaterally toward the apex of the axilla; hence it is often called the axillary border. The lateral border is made up of a thick bar of bone that prevents buckling of this stress-bearing region of the scapula.
The lateral border terminates in the truncated lateral angle of the scapula, the thickest part of the bone that bears the broadened head of the scapula (Fig. 6.5A & B). The glenoid cavity is the primary feature of the head. The shallow constriction between the head and body defines the neck of the scapula. The superior border of the scapula is marked near the junction of its medial two thirds and lateral third by the suprascapular notch, which is located where the superior border joins the base of the coracoid process. The superior border is the thinnest and shortest of the three borders.
The scapula is capable of considerable movement on the thoracic wall at the physiological scapulothoracic joint, providing the base from which the upper limb operates. These movements, enabling the arm to move freely, are discussed later in this chapter with the muscles that move the scapula.
Humerus
The humerus (arm bone), the largest bone in the upper limb, articulates with the scapula at the glenohumeral joint, and the radius and ulna at the elbow joint (Figs. 6.1, 6.3, and 6.5C). The proximal end of the humerus has a head, surgical and anatomical necks, and greater and lesser tubercles. The spherical head of the humerus articulates with the glenoid cavity of the scapula. The anatomical neck of the humerus is formed by the groove circumscribing the head and separating it from the greater and lesser tubercles. It indicates the line of attachment of the glenohumeral joint capsule. The surgical neck of the humerus, a common site of fracture, is the narrow part distal to the head and tubercles (Fig. 6.3B).
The junction of the head and neck with the shaft of the humerus is indicated by the greater and lesser tubercles, which provide attachment and leverage to some scapulohumeral muscles (Fig. 6.3A & B). The greater tubercle is at the lateral margin of the humerus, whereas the lesser tubercle projects anteriorly from the bone. The intertubercular sulcus (bicipital groove) separates the tubercles, and provides protected passage for the slender tendon of the long head of the biceps muscle.
The shaft of the humerus has two prominent features: the deltoid tuberosity laterally, for attachment of the deltoid muscle, and the oblique radial groove (groove for radial nerve, spiral groove) posteriorly, in which the radial nerve and profunda brachii artery lie as they pass anterior to the long head and between the medial and the lateral heads of the triceps brachii muscle. The inferior end of the humeral shaft widens as the sharp medial and lateral supra-epicondylar (supracondylar) ridges form, and then end distally in the especially prominent medial epicondyle and the lateral epicondyle, providing for muscle attachment.
The distal end of the humerus—including the trochlea, capitulum, olecranon, coronoid, and radial fossae—makes up the condyle of the humerus (Fig. 6.6). The condyle has two articular surfaces: a lateral capitulum (L. little head) for articulation with the head of the radius, and a medial, spool-shaped or pulley-like trochlea (L. pulley) for articulation with the proximal end (trochlear notch) of the ulna. Two hollows, or fossae, occur back to back superior to the trochlea, making the condyle quite thin between the epicondyles. Anteriorly, the coronoid fossa receives the coronoid process of the ulna during full flexion of the elbow. Posteriorly, the olecranon fossa accommodates the olecranon of the ulna during full extension of the elbow. Superior to the capitulum anteriorly, a shallower radial fossa accommodates the edge of the head of the radius when the forearm is fully flexed.

FIGURE 6.6. Distal end of right humerus. A and B. The condyle (the boundaries of which are indicated by the dashed line) consists of the capitulum; the trochlea; and the radial, coronoid, and olecranon fossae.
Bones of Forearm
The two forearm bones serve together to form the second unit of an articulated mobile strut (the first unit being the humerus), with a mobile base formed by the shoulder, that positions the hand. However, because this unit is formed by two parallel bones, one of which (the radius) can pivot about the other (the ulna), supination and pronation are possible. This makes it possible to rotate the hand when the elbow is flexed.
ULNA
The ulna is the stabilizing bone of the forearm and is the medial and longer of the two forearm bones (Figs. 6.7 and 6.8). Its more massive proximal end is specialized for articulation with the humerus proximally, and the head of the radius laterally. For articulation with the humerus, the ulna has two prominent projections: (1) the olecranon, which projects proximally from its posterior aspect (forming the point of the elbow), and serves as a short lever for extension of the elbow, and (2) the coronoid process, which projects anteriorly.

FIGURE 6.7. Bones of right elbow region. A. The proximal part of the ulna. B. The bones of the elbow region, demonstrating the relationship of the distal humerus and proximal ulna and radius during extension of the elbow joint. C. The relationship of the humerus and forearm bones during flexion of the elbow joint.

FIGURE 6.8. Right radius and ulna. A and B. The radius and ulna are shown in the articulated position, connected by the interosseous membrane. C and D. The features of the distal ends of the forearm bones. E. In cross section, the shafts of the radius and ulna appear almost as mirror images of one another for much of the middle and distal thirds of their lengths.
The olecranon and coronoid processes form the walls of the trochlear notch, which in profile resembles the jaws of a crescent wrench as it “grips” (articulates with) the trochlea of the humerus (Fig. 6.7B & C). The articulation between the ulna and humerus primarily allows only flexion and extension of the elbow joint, although a small amount of abduction–adduction occurs during pronation and supination of the forearm. Inferior to the coronoid process is the tuberosity of the ulna for attachment of the tendon of the brachialis muscle (Fig. 6.7A and 6.8A & B).
On the lateral side of the coronoid process is a smooth, rounded concavity, the radial notch, which receives the broad periphery of the head of the radius. Inferior to the radial notch on the lateral surface of the ulnar shaft is a prominent ridge, the supinator crest. Between it and the distal part of the coronoid process is a concavity, the supinator fossa. The deep part of the supinator muscle attaches to the supinator crest and fossa (6.7A).
The shaft of the ulna is thick and cylindrical proximally, but it tapers, diminishing in diameter, as it continues distally (Fig. 6.8A). At the narrow distal end of the ulna is a small but abrupt enlargement, the disc-like head of the ulna with a small, conical ulnar styloid process. The ulna does not reach—and therefore does not participate in—the wrist (radiocarpal) joint (Fig. 6.8).
RADIUS
The radius is the lateral and shorter of the two forearm bones. Its proximal end includes a short head, neck, and medially directed tuberosity (Fig. 6.8A). Proximally, the smooth superior aspect of the discoid head of the radius is concave for articulation with the capitulum of the humerus during flexion and extension of the elbow joint. The head also articulates peripherally with the radial notch of the ulna; thus the head is covered with articular cartilage.
The neck of the radius is a constriction distal to the head. The oval radial tuberosity is distal to the medial part of the neck, and demarcates the proximal end (head and neck) of the radius from the shaft.
The shaft of the radius, in contrast to that of the ulna, gradually enlarges as it passes distally. The distal end of the radius is essentially four sided when sectioned transversely. Its medial aspect forms a concavity, the ulnar notch (Fig. 6.8C & D), which accommodates the head of the ulna. Its lateral aspect becomes increasingly ridge-like, terminating distally in the radial styloid process.
Projecting dorsally, the dorsal tubercle of the radius lies between otherwise shallow grooves for the passage of the tendons of forearm muscles. The radial styloid process is larger than the ulnar styloid process, and extends farther distally (Fig. 6.8A & B). This relationship is of clinical importance when the ulna and/or the radius is fractured.
Most of the length of the shafts of the radius and ulna are essentially triangular in cross section, with a rounded, superficially directed base and an acute, deeply directed apex (Fig. 6.8A & E). The apex is formed by a section of the sharp interosseous border of the radius or ulna that connects to the thin, fibrous interosseous membrane of the forearm (Fig. 6.8A, B, & E). The majority of the fibers of the interosseous membrane run an oblique course, passing inferiorly from the radius as they extend medially to the ulna (Fig. 6.8A & B). Thus, they are positioned to transmit forces received by the radius (via the hands) to the ulna for transmission to the humerus.
Bones of Hand
The wrist, or carpus, is composed of eight carpal bones, arranged in proximal and distal rows of four (Fig. 6.9A–C). These small bones give flexibility to the wrist. The carpus is markedly convex from side to side posteriorly, and concave anteriorly. Augmenting movement at the wrist joint, the two rows of carpal bones glide on each other; in addition, each bone glides on those adjacent to it.

FIGURE 6.9. Bones of right hand. A–C. The skeleton of the hand consists of three segments: the carpals of the wrist (subdivided into proximal and distal rows), the metacarpals of the palm, and the phalanges of the fingers or digits. U, ulna; R, radius. D. The distal end of the forearm and hand of a 2.5-year-old child. Ossification centers of only four carpal bones are visible. Observe the distal radial epiphysis (R). E. The distal end of the forearm and hand of an 11-year-old child. Ossification centers of all carpal bones are visible. The arrow indicates the pisiform lying on the anterior surface of the triquetrum. The distal epiphysis of the ulna has ossified, but all the epiphyseal plates (lines) remain open (i.e., they are still unossified). (Parts C and D courtesy of Dr. D. Armstrong, Associate Professor of Medical Imaging, University of Toronto, Toronto, Ontario, Canada.).
From lateral to medial, the four carpal bones in the proximal row (purple in Fig. 6.9A & B) are the:
• Scaphoid (G. skaphé, skiff, boat): a boat-shaped bone that articulates proximally with the radius, and has a prominent scaphoid tubercle; it is the largest bone in the proximal row of carpals.
• Lunate (L. luna, moon): a moon-shaped bone between the scaphoid and the triquetral bones; it articulates proximally with the radius and is broader anteriorly than posteriorly.
• Triquetrum (L. triquetrus, three-cornered): a pyramidal bone on the medial side of the carpus; it articulates proximally with the articular disc of the distal radio-ulnar joint.
• Pisiform (L. pisum, pea), a small, pea-shaped bone that lies on the palmar surface of the triquetrum.
From lateral to medial, the four carpal bones in the distal row (green in Fig. 6.9A & B) are the:
• Trapezium (G. trapeze, table): a four-sided bone on the lateral side of the carpus; it articulates with the 1st and 2nd metacarpals, scaphoid, and trapezoid bones.
• Trapezoid: a wedge-shaped bone that resembles the trapezium; it articulates with the 2nd metacarpal, trapezium, capitate, and scaphoid bones.
• Capitate (L. caput, head): a head-shaped bone with a rounded extremity is the largest bone in the carpus; it articulates primarily with the 3rd metacarpal distally, and with the trapezoid, scaphoid, lunate, and hamate.
• Hamate (L. hamulus, a little hook): a wedge-shaped bone on the medial side of the hand; it articulates with the 4th and 5th metacarpal, capitate, and triquetral bones; it has a distinctive hooked process, the hook of the hamate, that extends anteriorly.
The proximal surfaces of the distal row of carpal bones articulate with the proximal row of carpal bones, and their distal surfaces articulate with the metacarpals.
The metacarpus forms the skeleton of the palm of the hand between the carpus and the phalanges. It is composed of five metacarpal bones (metacarpals). Each metacarpal consists of a base, shaft, and head. The proximal bases of the metacarpals articulate with the carpal bones, and the distal heads of the metacarpals articulate with the proximal phalanges, and form the knuckles of the hand. The 1st metacarpal (of the thumb) is the thickest and shortest of these bones. The 3rd metacarpal is distinguished by a styloid process on the lateral side of its base (Fig. 6.10).

FIGURE 6.10. Surface anatomy of bones of upper limb.
Each digit (finger) has three phalanges except for the first (the thumb), which has only two; however, the phalanges of the first digit are stouter than those in the other fingers. Each phalanx has a base proximally, a shaft (body), and a head distally (Fig. 6.9). The proximal phalanges are the largest, the middle ones are intermediate in size, and the distal ones are the smallest. The shafts of the phalanges taper distally. The terminal phalanges are flattened and expanded at their distal ends, which underlie the nail beds.
OSSIFICATION OF BONES OF HAND
Radiographs of the wrist and hand are commonly used to assess skeletal age. For clinical studies, the radiographs are compared with a series of standards in a radiographic atlas of skeletal development to determine the skeletal age. Ossification centers are usually obvious during the 1st year; however, they may appear before birth. Each carpal bone usually ossifies from one center postnatally (Fig. 6.9D). The centers for the capitate and hamate appear first.
The shaft of each metacarpal begins to ossify during fetal life, and ossification centers appear postnatally in the heads of the four medial metacarpals and in the base of the 1st metacarpal. By age 11, ossification centers of all carpal bones are visible (Fig. 6.9E).
Surface Anatomy of Upper Limb Bones
Most bones of the upper limb offer a palpable segment or surface (notable exceptions being the lunate and trapezoid), enabling the skilled examiner to discern abnormalities owing to trauma (fracture or dislocation) or malformation (Fig. 6.10).
The clavicle is subcutaneous and can be easily palpated throughout its length. Its sternal end projects superior to the manubrium (Fig. 6.10). Between the elevated sternal ends of the clavicles is the jugular notch (suprasternal notch). The acromial end of the clavicle often rises higher than the acromion, forming a palpable elevation at the acromioclavicular (AC) joint. The acromial end can be palpated 2–3 cm medial to the lateral border of the acromion, particularly when the arm is alternately flexed and extended. Either or both ends of the clavicle may be prominent; when present, this condition is usually bilateral.
Note the elasticity of the skin over the clavicle and how easily it can be pinched into a mobile fold. This property of the skin is useful when ligating (tying a knot around) the third part of the subclavian artery: The skin lying superior to the clavicle is pulled down onto the clavicle and then incised; after the incision is made, the skin is allowed to return to its position superior to the clavicle, where it overlies the artery (thus not endangering it during the incision).
As the clavicle passes laterally, its medial part can be felt to be convex anteriorly. The large vessels and nerves to the upper limb pass posterior to this convexity. The flattened acromial end of the clavicle does not reach the point of the shoulder, formed by the lateral tip of the acromion of the scapula.
The acromion of the scapula is easily felt and often visible, especially when the deltoid contracts against resistance. The superior surface of the acromion is subcutaneous and may be traced medially to the AC joint. The lateral and posterior borders of the acromion meet to form the acromial angle (Fig. 6.10B). The humerus in the glenoid cavity and the deltoid muscle form the rounded curve of the shoulder. The crest of the scapular spine is subcutaneous throughout and easily palpated.
When the upper limb is in the anatomical position, the:
• Superior angle of the scapula lies at the level of the T2 vertebra.
• Medial end of the root of the scapular spine is opposite the spinous process of the T3 vertebra.
• Inferior angle of the scapula lies at the level of the T7 vertebra, near the inferior border of the 7th rib and 7th intercostal space.
The medial border of the scapula is palpable inferior to the root of the spine of the scapula as it crosses the 3rd–7th ribs. The lateral border of the scapula is not easily palpated because it is covered by the teres major and minor muscles. When the upper limb is abducted and the hand is placed on the back of the head, the scapula is rotated, elevating the glenoid cavity such that the medial border of the scapula parallels the 6th rib and thus can be used to estimate its position and, deep to the rib, the oblique fissure of the lung. The inferior angle of the scapula is easily felt and is often visible. It is grasped when testing movements of the glenohumeral joint to immobilize the scapula. The coracoid process of the scapula can be felt by palpating deeply at the lateral side of the clavipectoral (deltopectoral) triangle (Fig. 6.11).

FIGURE 6.11. Palpation of coracoid process of scapula.
The head of the humerus is surrounded by muscles, except inferiorly; consequently, it can be palpated only by pushing the fingers well up into the axillary fossa (armpit). The arm should not be fully abducted, otherwise the fascia in the axilla will be tense and impede palpation of the humeral head. When the arm is moved and the scapula is fixed (held in place), the head of the humerus can be palpated.
The greater tubercle of the humerus may be felt with the person’s arm by the side on deep palpation through the deltoid, inferior to the lateral border of the acromion. In this position, the greater tubercle is the most lateral bony point of the shoulder and, along with the deltoid, gives the shoulder its rounded contour. When the arm is abducted, the greater tubercle is pulled beneath the acromion and is no longer palpable.
The lesser tubercle of the humerus may be felt with difficulty by deep palpation through the deltoid on the anterior aspect of the arm, approximately 1 cm lateral and slightly inferior to the tip of the coracoid process. Rotation of the arm facilitates palpation of this tubercle. The location of the intertubercular sulcus or bicipital groove, between the greater and the lesser tubercles, is identifiable during flexion and extension of the elbow joint by palpating in an upward direction along the tendon of the long head of the biceps brachii as it moves through the intertubercular groove.
The shaft of the humerus may be felt with varying distinctness through the muscles surrounding it. No part of the proximal part of the humeral shaft is subcutaneous.
The medial and lateral epicondyles of the humerus are subcutaneous and easily palpated on the medial and lateral aspects of the elbow region. The knob-like medial epicondyle, projecting posteromedially, is more prominent than the lateral epicondyle.
When the elbow joint is partially flexed, the lateral epicondyle is visible. When the elbow joint is fully extended, the lateral epicondyle can be palpated but not seen deep to a depression on the posterolateral aspect of the elbow.
The olecranon of the ulna can be easily palpated (Fig. 6.12). When the elbow joint is extended, observe that the tip of the olecranon and the humeral epicondyles lie in a straight line (Fig. 6.12A & B). When the elbow is flexed, the olecranon descends until its tip forms the apex of an approximately equilateral triangle, of which the epicondyles form the angles at its base (Fig. 6.12C). These normal relationships are important in the diagnosis of certain elbow injuries (e.g., dislocation of the elbow joint).

FIGURE 6.12. Surface anatomy of bones and bony formations of elbow region.
The posterior border of the ulna, palpable throughout the length of the forearm, demarcates the posteromedial boundary between the flexor–pronator and the extensor–supinator compartments of the forearm. The head of the ulna forms a large, rounded subcutaneous prominence that can be easily seen and palpated on the medial side of the dorsal aspect of the wrist, especially when the hand is pronated. The pointed subcutaneous ulnar styloid process may be felt slightly distal to the rounded ulnar head when the hand is supinated.
The head of the radius can be palpated and felt to rotate in the depression on the posterolateral aspect of the extended elbow joint, just distal to the lateral epicondyle of the humerus. The radial head can also be palpated as it rotates during pronation and supination of the forearm. The ulnar nerve feels like a thick cord where it passes posterior to the medial epicondyle of the humerus; pressing the nerve here evokes an unpleasant “funny bone” sensation.
The radial styloid process can be easily palpated in the anatomical snuff box on the lateral side of the wrist (see Fig. 6.65A); it is larger and approximately 1 cm more distal than the ulnar styloid process. The radial styloid process is easiest to palpate when the thumb is abducted. It is overlaid by the tendons of the thumb muscles. Because the radial styloid process extends more distally than the ulnar styloid process, more ulnar deviation than radial deviation of the wrist is possible.

FIGURE 6.65. Anatomical snuff box. A. When the thumb is extended, a triangular hollow appears between the tendon of the extensor pollicis longus (EPL) medially and the tendons of the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) laterally. B. The floor of the snuff box, formed by the scaphoid and trapezium bones, is crossed by the radial artery as it passes diagonally from the anterior surface of the radius to the dorsal surface of the hand.
The relationship of the radial and ulnar styloid processes is important in the diagnosis of certain wrist injuries (e.g., Colles fracture). Proximal to the radial styloid process, the anterior, lateral, and posterior surfaces of the radius are palpable for several centimeters. The dorsal tubercle of radius is easily felt around the middle of the dorsal aspect of the distal end of the radius. The dorsal tubercle acts as a pulley for the long extensor tendon of the thumb, which passes medial to it.
The pisiform can be felt on the anterior aspect of the medial border of the wrist and can be moved from side to side when the hand is relaxed. The hook of the hamate can be palpated on deep pressure over the medial side of the palm, approximately 2 cm distal and lateral to the pisiform. The tubercles of the scaphoid and trapezium can be palpated at the base and medial aspect of the thenar eminence (ball of thumb) when the hand is extended.
The metacarpals, although overlain by the long extensor tendons of the digits, can be palpated on the dorsum of the hand. The heads of these bones form the knuckles of the fist; the 3rd metacarpal head is most prominent. The styloid process of the 3rd metacarpal can be palpated approximately 3.5 cm from the dorsal tubercle of radius. The dorsal aspects of the phalanges can also be easily palpated. The knuckles of the fingers are formed by the heads of the proximal and middle phalanges.
When measuring the upper limb, or segments of it, for comparison with the contralateral limb, or with standards for normal limb growth or size, the acromial angle (Fig. 6.10B), lateral epicondyle of the humerus, styloid process of the radius, and tip of the third digit are most commonly used as measuring points, with the limb relaxed (dangling), but with palms directed anteriorly.
BONES OF UPPER LIMB
Upper Limb Injuries
 Because the disabling effects of an injury to an upper limb, particularly the hand, are far out of proportion to the extent of the injury, a sound understanding of the structure and function of the upper limb is of the highest importance. Knowledge of its structure without an understanding of its functions is almost useless clinically because the aim of treating an injured limb is to preserve or restore its functions.
Because the disabling effects of an injury to an upper limb, particularly the hand, are far out of proportion to the extent of the injury, a sound understanding of the structure and function of the upper limb is of the highest importance. Knowledge of its structure without an understanding of its functions is almost useless clinically because the aim of treating an injured limb is to preserve or restore its functions.
Variations of Clavicle
 The clavicle varies more in shape than most other long bones. Occasionally, the clavicle is pierced by a branch of the supraclavicular nerve. The clavicle is thicker and more curved in manual workers, and the sites of muscular attachments are more marked.
The clavicle varies more in shape than most other long bones. Occasionally, the clavicle is pierced by a branch of the supraclavicular nerve. The clavicle is thicker and more curved in manual workers, and the sites of muscular attachments are more marked.
Fracture of Clavicle
 The clavicle is one of the most frequently fractured bones. Clavicular fractures are especially common in children, and are often caused by an indirect force transmitted from an outstretched hand through the bones of the forearm and arm to the shoulder during a fall. A fracture may also result from a fall directly on the shoulder. The weakest part of the clavicle is the junction of its middle and lateral thirds.
The clavicle is one of the most frequently fractured bones. Clavicular fractures are especially common in children, and are often caused by an indirect force transmitted from an outstretched hand through the bones of the forearm and arm to the shoulder during a fall. A fracture may also result from a fall directly on the shoulder. The weakest part of the clavicle is the junction of its middle and lateral thirds.
After fracture of the clavicle, the sternocleidomastoid muscle elevates the medial fragment of bone (Fig. B6.1). Because of the subcutaneous position of the clavicle, the end of the superiorly directed fragment is prominent—readily palpable and/or apparent. The trapezius muscle is unable to hold the lateral fragment up owing to the weight of the upper limb; thus, the shoulder drops. The strong coracoclavicular ligament usually prevents dislocation of the acromioclavicular (AC) joint. People with fractured clavicles support the sagging limb with the other limb. In addition to being depressed, the lateral fragment of the clavicle may be pulled medially by the adductor muscles of the arm, such as the pectoralis major. Overriding of the bone fragments shortens the clavicle.

FIGURE B6.1. Fracture of clavicle.
The slender clavicles of neonates may be fractured during delivery if they have broad shoulders; however, the bones usually heal quickly. A fracture of the clavicle is often incomplete in younger children—that is, it is a greenstick fracture, in which one side of a bone is broken and the other is bent. This fracture was so named because the parts of the bone do not separate; the bone resembles a tree branch (greenstick) that has been sharply bent but not disconnected.
Ossification of Clavicle
 The clavicle is the first long bone to ossify (via intramembranous ossification), beginning during the 5th and 6th embryonic weeks from medial and lateral primary ossification centers that are close together in the shaft of the clavicle. The ends of the clavicle later pass through a cartilaginous phase (endochondral ossification); the cartilages form growth zones similar to those of other long bones. A secondary ossification center appears at the sternal end, and forms a scale-like epiphysis that begins to fuse with the shaft (diaphysis) between 18 and 25 years of age, and is completely fused to it between 25 and 31 years of age. This is the last of the epiphyses of long bones to fuse. An even smaller scale-like epiphysis may be present at the acromial end of the clavicle; it must not be mistaken for a fracture.
The clavicle is the first long bone to ossify (via intramembranous ossification), beginning during the 5th and 6th embryonic weeks from medial and lateral primary ossification centers that are close together in the shaft of the clavicle. The ends of the clavicle later pass through a cartilaginous phase (endochondral ossification); the cartilages form growth zones similar to those of other long bones. A secondary ossification center appears at the sternal end, and forms a scale-like epiphysis that begins to fuse with the shaft (diaphysis) between 18 and 25 years of age, and is completely fused to it between 25 and 31 years of age. This is the last of the epiphyses of long bones to fuse. An even smaller scale-like epiphysis may be present at the acromial end of the clavicle; it must not be mistaken for a fracture.
Sometimes fusion of the two ossification centers of the clavicle fails to occur; as a result, a bony defect forms between the lateral and medial thirds of the clavicle. Awareness of this possible congenital defect should prevent diagnosis of a fracture in an otherwise normal clavicle. When doubt exists, both clavicles are radiographed because this defect is usually bilateral (Ger et al., 1996).
Fracture of Scapula
 Fracture of the scapula is usually the result of severe trauma, as occurs in pedestrian–vehicle accidents. Usually there are also fractured ribs. Most fractures require little treatment because the scapula is covered on both sides by muscles. Most fractures involve the protruding subcutaneous acromion.
Fracture of the scapula is usually the result of severe trauma, as occurs in pedestrian–vehicle accidents. Usually there are also fractured ribs. Most fractures require little treatment because the scapula is covered on both sides by muscles. Most fractures involve the protruding subcutaneous acromion.
Fractures of Humerus
 Most injuries of the proximal end of the humerus are fractures of the surgical neck. These injuries are especially common in elderly people with osteoporosis, whose demineralized bones are brittle. Humeral fractures often result in one fragment being driven into the spongy bone of the other fragment (impacted fracture). The injuries usually result from a minor fall on the hand, with the force being transmitted up the forearm bones of the extended limb. Because of impaction of the fragments, the fracture site is sometimes stable and the person is able to move the arm passively with little pain.
Most injuries of the proximal end of the humerus are fractures of the surgical neck. These injuries are especially common in elderly people with osteoporosis, whose demineralized bones are brittle. Humeral fractures often result in one fragment being driven into the spongy bone of the other fragment (impacted fracture). The injuries usually result from a minor fall on the hand, with the force being transmitted up the forearm bones of the extended limb. Because of impaction of the fragments, the fracture site is sometimes stable and the person is able to move the arm passively with little pain.
An avulsion fracture of the greater tubercle of the humerus is seen most commonly in middle-aged and elderly people (Fig. B6.2A). A small part of the tubercle is “avulsed” (torn away). The fracture usually results from a fall on the acromion, the point of the shoulder. In younger people, an avulsion fracture of the greater tubercle usually results from a fall on the hand when the arm is abducted. Muscles (especially the subscapularis) that remain attached to the humerus pull the limb into medial rotation.

FIGURE B6.2. Humeral fractures. A. An avulsion fracture of the greater tubercle of the humerus. B. A transverse fracture of humeral body.
A transverse fracture of the shaft of the humerus frequently results from a direct blow to the arm. The pull of the deltoid muscle carries the proximal fragment laterally (Fig. B6.2B). Indirect injury resulting from a fall on the outstretched hand may produce a spiral fracture of the humeral shaft. Overriding of the oblique ends of the fractured bone may result in foreshortening. Because the humerus is surrounded by muscles and has a well-developed periosteum, the bone fragments usually unite well.
An intercondylar fracture of the humerus results from a severe fall on the flexed elbow. The olecranon of the ulna is driven like a wedge between the medial and lateral parts of the condyle of the humerus, separating one or both parts from the humeral shaft.
The following parts of the humerus are in direct contact with the indicated nerves:
• Surgical neck: axillary nerve.
• Radial groove: radial nerve.
• Distal end of humerus: median nerve.
• Medial epicondyle: ulnar nerve.
These nerves may be injured when the associated part of the humerus is fractured. These injuries are discussed later in this chapter.
Fractures of Radius and Ulna
 Fractures of both the radius and the ulna are usually the result of severe injury. A direct injury usually produces transverse fractures at the same level, usually in the middle third of the bones. Isolated fractures of the radius or ulna also occur. Because the shafts of these bones are firmly bound together by the interosseous membrane, a fracture of one bone is likely to be associated with dislocation of the nearest joint.
Fractures of both the radius and the ulna are usually the result of severe injury. A direct injury usually produces transverse fractures at the same level, usually in the middle third of the bones. Isolated fractures of the radius or ulna also occur. Because the shafts of these bones are firmly bound together by the interosseous membrane, a fracture of one bone is likely to be associated with dislocation of the nearest joint.
Fracture of the distal end of the radius is a common fracture in adults > 50 years of age, and occurs more frequently in women because their bones are more commonly weakened by osteoporosis. A complete transverse fracture of the distal 2 cm of the radius, called a Colles fracture, is the most common fracture of the forearm (Fig. B6.3). The distal fragment is displaced dorsally and is often comminuted (broken into pieces). The fracture results from forced extension of the hand, usually as the result of trying to ease a fall by outstretching the upper limb.

FIGURE B6.3. Distal fracture of forearm bones. A. A normal wrist. B. A Colles fracture with a dinner fork deformity.
Often the ulnar styloid process is avulsed (broken off). Normally the radial styloid process projects farther distally than the ulnar styloid (Fig. B6.3A); consequently, when a Colles fracture occurs, this relationship is reversed because of shortening of the radius (Fig. B6.3B). This fracture is often referred to as a dinner fork deformity because a posterior angulation occurs in the forearm just proximal to the wrist and the normal anterior curvature of the relaxed hand. The posterior bending is produced by the posterior displacement and tilt of the distal fragment of the radius.
The typical history of a person with a Colles fracture includes slipping or tripping and, in an attempt to break the fall, landing on the outstretched limb with the forearm and hand pronated. Because of the rich blood supply to the distal end of the radius, bony union is usually good.
When the distal end of the radius fractures in children, the fracture line may extend through the distal epiphysial plate. Epiphysial plate injuries are common in older children because of their frequent falls in which the forces are transmitted from the hand to the radius and ulna. The healing process may result in malalignment of the epiphysial plate and disturbance of radial growth.
Fracture of Scaphoid
 The scaphoid is the most frequently fractured carpal bone. It often results from a fall on the palm when the hand is abducted, the fracture occurring across the narrow part of the scaphoid (Fig. B6.4). Pain occurs primarily on the lateral side of the wrist, especially during dorsiflexion and abduction of the hand. Initial radiographs of the wrist may not reveal a fracture; often this injury is (mis)diagnosed as a severely sprained wrist.
The scaphoid is the most frequently fractured carpal bone. It often results from a fall on the palm when the hand is abducted, the fracture occurring across the narrow part of the scaphoid (Fig. B6.4). Pain occurs primarily on the lateral side of the wrist, especially during dorsiflexion and abduction of the hand. Initial radiographs of the wrist may not reveal a fracture; often this injury is (mis)diagnosed as a severely sprained wrist.

FIGURE B6.4. Fracture of scaphoid.
Radiographs taken 10–14 days later reveal a fracture because bone resorption has occurred there. Owing to the poor blood supply to the proximal part of the scaphoid, union of the fractured parts may take at least 3 months. Avascular necrosis of the proximal fragment of the scaphoid (pathological death of bone, resulting from inadequate blood supply) may occur, and produce degenerative joint disease of the wrist. In some cases, it is necessary to fuse the carpals surgically (arthrodesis).
Fracture of Hamate
 Fracture of the hamate may result in non-union of the fractured bony parts because of the traction produced by the attached muscles. Because the ulnar nerve is close to the hook of the hamate, the nerve may be injured by this fracture, causing decreased grip strength of the hand. The ulnar artery may also be damaged when the hamate is fractured.
Fracture of the hamate may result in non-union of the fractured bony parts because of the traction produced by the attached muscles. Because the ulnar nerve is close to the hook of the hamate, the nerve may be injured by this fracture, causing decreased grip strength of the hand. The ulnar artery may also be damaged when the hamate is fractured.
Fracture of Metacarpals
 The metacarpals (except the 1st) are closely bound together; hence isolated fractures tend to be stable. Furthermore, these bones have a good blood supply, and fractures usually heal rapidly. Severe crushing injuries of the hand may produce multiple metacarpal fractures, resulting in instability of the hand. Fracture of the 5th metacarpal, often referred to as a boxer’s fracture, occurs when an unskilled person punches someone with a closed and abducted fist. The head of the bone rotates over the distal end of the shaft, producing a flexion deformity.
The metacarpals (except the 1st) are closely bound together; hence isolated fractures tend to be stable. Furthermore, these bones have a good blood supply, and fractures usually heal rapidly. Severe crushing injuries of the hand may produce multiple metacarpal fractures, resulting in instability of the hand. Fracture of the 5th metacarpal, often referred to as a boxer’s fracture, occurs when an unskilled person punches someone with a closed and abducted fist. The head of the bone rotates over the distal end of the shaft, producing a flexion deformity.
Fracture of Phalanges
 Crushing injuries of the distal phalanges are common (e.g., when a finger is caught in a car door). Because of the highly developed sensation in the fingers, these injuries are extremely painful. A fracture of a distal phalanx is usually comminuted, and a painful hematoma (local collection of blood) soon develops. Fractures of the proximal and middle phalanges are usually the result of crushing or hyperextension injuries. Because of the close relationship of phalangeal fractures to the flexor tendons, the bone fragments must be carefully realigned to restore normal function of the fingers.
Crushing injuries of the distal phalanges are common (e.g., when a finger is caught in a car door). Because of the highly developed sensation in the fingers, these injuries are extremely painful. A fracture of a distal phalanx is usually comminuted, and a painful hematoma (local collection of blood) soon develops. Fractures of the proximal and middle phalanges are usually the result of crushing or hyperextension injuries. Because of the close relationship of phalangeal fractures to the flexor tendons, the bone fragments must be carefully realigned to restore normal function of the fingers.
The Bottom Line
BONES OF UPPER LIMB
Comparison of upper and lower limbs: The development and structure of the upper and lower limbs have much in common; however, the upper limb has become a mobile organ that allows humans not only to respond to their environment, but to manipulate and control it to a large degree. ♦ The upper limb is composed of four increasingly mobile segments: The proximal three (shoulder, arm, and forearm) serve primarily to position the fourth segment (hand), which is used for grasping, manipulation, and touch. ♦ Four characteristics allow the independent operation of the upper limbs, allowing the hands to be precisely positioned and enabling accurate eye–hand coordination: (1) the upper limbs are not involved in weight bearing or ambulation, (2) the pectoral girdle is attached to the axial skeleton only anteriorly via a very mobile joint, (3) paired bones of the forearm can be moved relative to each other, and (4) the hands have long, mobile fingers and an opposable thumb.
Clavicle: The subcutaneously-located clavicle connects the upper limb (superior appendicular skeleton) to the trunk (axial skeleton). ♦ The clavicle serves as a movable crane-like strut (extended support) from which the scapula and free limb are suspended at a distance from the trunk that enables freedom of motion. ♦ Shocks received by the upper limb (especially the shoulder) are transmitted through the clavicle, resulting in a fracture that most commonly occurs between its middle and lateral thirds. ♦ The clavicle is the first long bone to ossify and the last to be fully formed.
Scapula: The scapula forms the mobile base from which the free upper limb acts. ♦ This triangular flat bone is curved to conform to the thoracic wall, and provides large surface areas and edges for attachment of muscles. ♦ These muscles (1) move the scapula on the thoracic wall at the physiological scapulothoracic joint, and (2) extend to the proximal humerus maintaining the integrity of—and producing motion at—the glenohumeral joint. ♦ The spine of the scapula and acromion serve as levers; the acromion enables the scapula and attached muscles to be located medially against the trunk with the acromioclavicular (AC) and glenohumeral joints, thereby allowing movement lateral to the trunk. ♦ The coracoid process of the scapula is the site of attachment for the coracoclavicular ligament, which passively supports the upper limb, and a site for muscular (tendon) attachment.
Humerus: The long, strong humerus is a mobile strut—the first in a series of two—used to position the hand at a height (level) and distance from the trunk to maximize its efficiency. ♦ The spherical head of the humerus enables a great range of motion on the mobile scapular base; the trochlea and capitulum at its distal end facilitate the hinge movements of the elbow and, at the same time, the pivoting of the radius. ♦ The long shaft of the humerus enables reaching, and makes it an effective lever for power in lifting, as well as providing surface area for attachment of muscles that act primarily at the elbow. ♦ Added surface area for attachment of flexors and extensors of the wrist is provided by the epicondyles, the medial and lateral extensions of the distal end of the humerus.
Ulna and radius: The ulna and radius together make up the second unit of a two-unit articulated strut (the first unit being the humerus), projecting from a mobile base (shoulder) that serves to position the hand. ♦ Because the forearm unit is formed by two parallel bones, and the radius is able to pivot about the ulna, supination and pronation of the hand are possible during elbow flexion. ♦ Proximally, the larger medial ulna forms the primary articulation with the humerus, whereas distally, the shorter lateral radius forms the primary articulation with the hand via the wrist. ♦ Because the ulna does not reach the wrist, forces received by the hand are transmitted from the radius to the ulna via the interosseous membrane.
Hand: Each segment of the upper limb increases the functionality of the end unit, the hand. ♦ Located on the free end of a two-unit articulated strut (arm and forearm) projecting from a mobile base (shoulder), the hand can be positioned over a wide range relative to the trunk. ♦ The hand’s connection to the flexible strut via the multiple small bones of the wrist, combined with the pivoting of the forearm, greatly increases its ability to be placed in a particular position with the digits able to flex (push or grip) in the necessary direction. ♦ The carpal bones are organized into two rows of four bones each and, as a group, articulate with the radius proximally and the metacarpals distally. ♦ The highly flexible, elongated digits—extending from a semirigid base (the palm)—enable the ability to grip, manipulate, or perform complex tasks involving multiple and simultaneous individual motions (e.g., when typing or playing a piano).
Surface anatomy: The upper limb presents multiple palpable bony features that are useful (1) when diagnosing fractures, dislocations, or malformations; (2) for approximating the position of deeper structures; and (3) for precisely describing the location of incisions and sites for therapeutic puncture, or areas of pathology or injury.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


