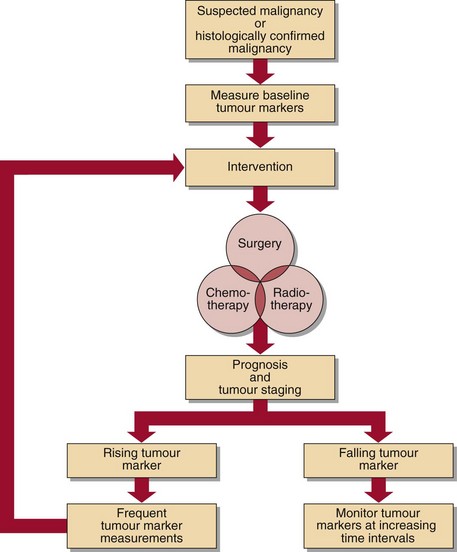
70 Tumour markers A tumour marker is any substance that can be related to the presence or progress of a tumour. In practice, the clinical biochemistry laboratory measures markers that are present in blood, although the term ‘tumour markers’ can also be applied to substances found on the surface of, or within, cells fixed in frozen or paraffin sections. A tumour marker in plasma has been secreted or released by the tumour cells. Such markers are not necessarily unique products of the malignant cells, but may simply be expressed by the tumour in a greater amount than by normal cells. Tumour markers fall into one of several groups: they may be hormones, e.g. human chorionic gonadotrophin (HCG) secreted by choriocarcinoma; or enzymes, e.g. prostate specific antigen (PSA) in prostate carcinoma; or tumour antigens, e.g. carcinoembryonic antigen (CEA) in colorectal carcinoma. The use of tumour markers Tumour markers can be used in different ways. They are of most value in monitoring treatment and assessing follow-up (Fig 70.1), but are also used in diagnosis, prognosis and screening for the presence of disease. Fig 70.1 The use of tumour markers. Monitoring treatment Treatment monitoring is the area in which most tumour markers have found a useful role. The decline in concentration of the tumour marker is an indication of the success of the treatment, whether that be surgery, chemotherapy, radiotherapy, or a combination of these. However, the rate of decline of marker concentration should match that predicted from knowledge of the marker’s half-life. A slower than expected fall may well indicate that not all the tumour has been eliminated. Assessing follow-up Even when a patient has had successful treatment, it is often valuable to continue to monitor the marker long after the levels have appeared to stabilize. An increase indicates recurrence of the malignancy. Detection of increasing marker concentration allows second-line therapy to be instituted promptly. The frequency of sampling, with the attendant cost implications, is much discussed. Diagnosis Markers alone are rarely used to establish a diagnosis. Their detection in blood when there is clinical evidence of the tumour as well as radiological and, perhaps, biopsy evidence, will often confirm the diagnosis. Prognosis Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: Hypernatraemia Liver function tests Hyperfunction of the adrenal cortex Hypothyroidism Stay updated, free articles. Join our Telegram channel Join Tags: Clinical Biochemistry An Illustrated Colour Text 5e Jun 18, 2016 | Posted by admin in BIOCHEMISTRY | Comments Off on Tumour markers Full access? Get Clinical Tree
70 Tumour markers A tumour marker is any substance that can be related to the presence or progress of a tumour. In practice, the clinical biochemistry laboratory measures markers that are present in blood, although the term ‘tumour markers’ can also be applied to substances found on the surface of, or within, cells fixed in frozen or paraffin sections. A tumour marker in plasma has been secreted or released by the tumour cells. Such markers are not necessarily unique products of the malignant cells, but may simply be expressed by the tumour in a greater amount than by normal cells. Tumour markers fall into one of several groups: they may be hormones, e.g. human chorionic gonadotrophin (HCG) secreted by choriocarcinoma; or enzymes, e.g. prostate specific antigen (PSA) in prostate carcinoma; or tumour antigens, e.g. carcinoembryonic antigen (CEA) in colorectal carcinoma. The use of tumour markers Tumour markers can be used in different ways. They are of most value in monitoring treatment and assessing follow-up (Fig 70.1), but are also used in diagnosis, prognosis and screening for the presence of disease. Fig 70.1 The use of tumour markers. Monitoring treatment Treatment monitoring is the area in which most tumour markers have found a useful role. The decline in concentration of the tumour marker is an indication of the success of the treatment, whether that be surgery, chemotherapy, radiotherapy, or a combination of these. However, the rate of decline of marker concentration should match that predicted from knowledge of the marker’s half-life. A slower than expected fall may well indicate that not all the tumour has been eliminated. Assessing follow-up Even when a patient has had successful treatment, it is often valuable to continue to monitor the marker long after the levels have appeared to stabilize. An increase indicates recurrence of the malignancy. Detection of increasing marker concentration allows second-line therapy to be instituted promptly. The frequency of sampling, with the attendant cost implications, is much discussed. Diagnosis Markers alone are rarely used to establish a diagnosis. Their detection in blood when there is clinical evidence of the tumour as well as radiological and, perhaps, biopsy evidence, will often confirm the diagnosis. Prognosis Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: Hypernatraemia Liver function tests Hyperfunction of the adrenal cortex Hypothyroidism Stay updated, free articles. Join our Telegram channel Join Tags: Clinical Biochemistry An Illustrated Colour Text 5e Jun 18, 2016 | Posted by admin in BIOCHEMISTRY | Comments Off on Tumour markers Full access? Get Clinical Tree