(1)
Department of Pathology, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
Keywords
Maxillofacial BonesChondroid TumorsChondrosarcomaChondromyxoid FibromaChondroblastoma10.1 Introduction
Cartilaginous tumors in the maxillofacial skeleton show the same features as their extragnathic counterparts. Chondroblastoma and chondromyxoid fibroma are very rare in the head and neck region. Chondrosarcoma is more frequently seen at this site but mainly in the walls of the sinonasal cavities, jaw location being uncommon. In this Chapter the clinicopathologic features of these tumors that have production of chondroid matrix as common feature are discussed.
10.2 Chondromyxoid Fibroma
Chondromyxoid fibroma is a benign tumor characterized by lobules of spindle-shaped or stellate cells with abundant myxoid or chondroid intercellular substance. The long bones are the sites most frequently affected, involvement of the skull and facial bones being less than 5 % [1]. Radiologically, they show an irregular radiolucency due to destruction of cancellous bone (Figs. 10.1 and 10.2).


Fig. 10.1
Chondromyxoid fibroma. Panoramic radiograph showing ill-defined radiolucency in right mandible together with resorption of the distal root of the mandibular first molar tooth
Fig. 10.2
Gross appearance of chondromyxoid fibroma showing diffuse spread in mandibular cancellous bone and limited demarcated expansion in adjacent soft tissues
The histologic features include the presence of stellate or spindle-shaped cells in a myxoid background, arranged in lobules (Fig. 10.3). The interlobular tissue is cellular and also composed of oval or spindle-shaped cells. Multinucleated giant cells may be present at the border of the lobules in approximately 50 % of tumors (Figs. 10.4 and 10.5). Calcification and/or hyaline cartilage is seen in a minority of cases (Fig. 10.6). Focally, nuclear atypia, binucleate cells and mitotic figures may be observed (Fig. 10.7) and metaplastic ossification may change the appearance of the chondroid matrix (Fig. 10.8). In some cases, the lobularity is not very conspicuous, the tumor only showing a diffuse proliferation of stellate-shaped cells in a loose myxoid background (Fig. 10.9). The lesion shows demarcation from adjacent soft tissues by an expanding and attenuated cortical rim but there is no demarcation between the tumor and adjacent cancellous bone in which the tumor may invade (Figs. 10.10 and 10.11).
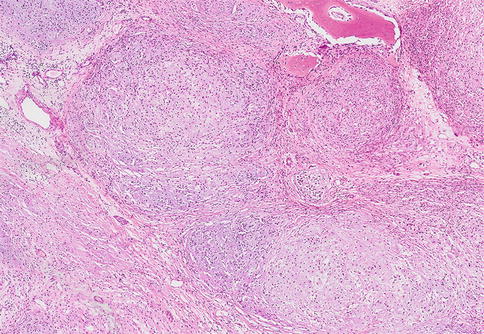
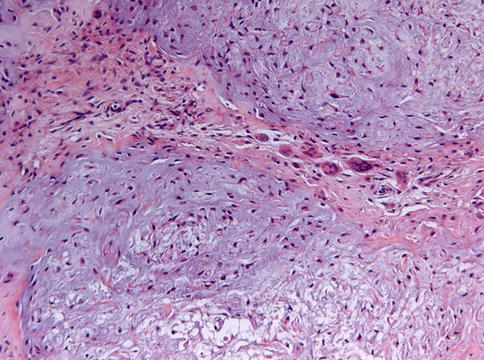
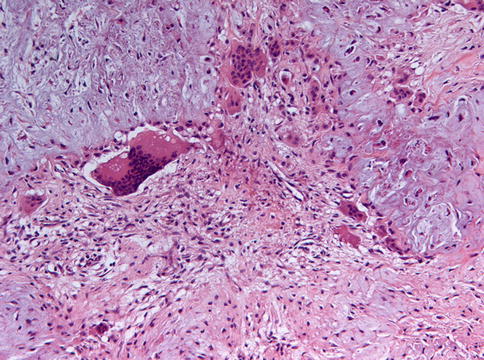
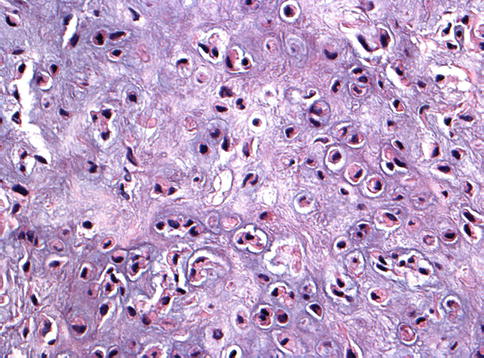
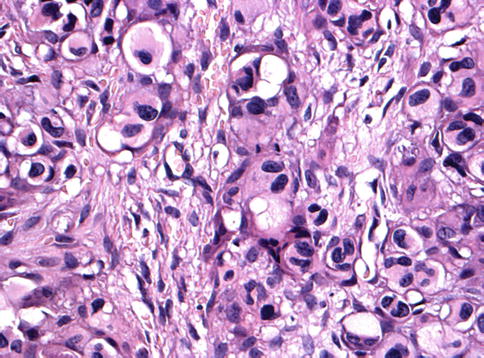
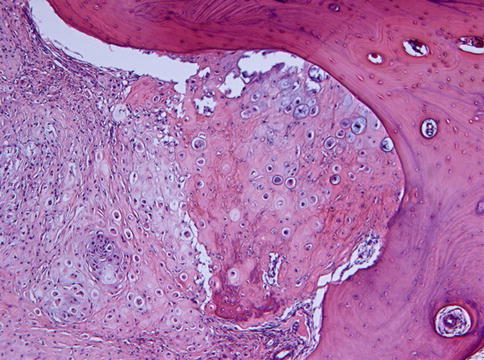
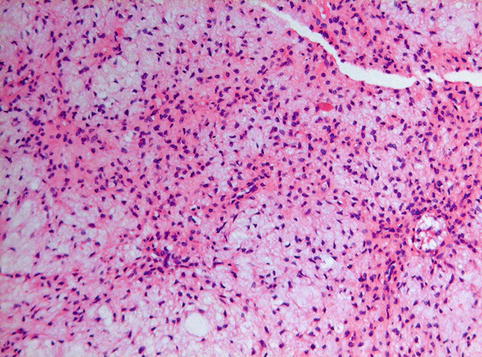

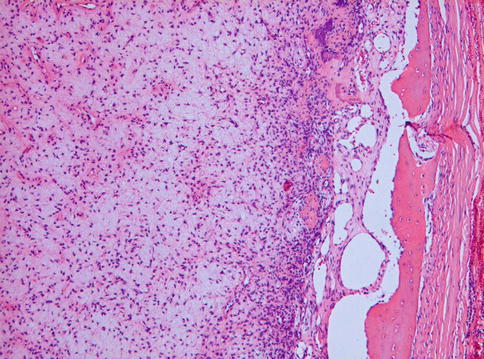
Fig. 10.3
Low power view of chondromyxoid fibroma to illustrate the lobular growth pattern
Fig. 10.4
Lobuli are composed of spindle cells. Multinucleated giant cells lying at the periphery of the lobules also are characteristic for chondromyxoid fibroma
Fig. 10.5
Higher magnification of Fig. 10.4 to highlight the multinucleated giant cells and the cytomorphology of the spindle cells. Some of them show a perinuclear halo indicating chondroid differentiation
Fig. 10.6
Occasionally, hyaline cartilage may form part of the histologic spectrum shown by chondromyxoid fibroma
Fig. 10.7
Focally, chondromyxoid fibroma may show cytonuclear atypia, binucleate cells, and mitotic activity that may cause confusion with chondrosarcoma
Fig. 10.8
Metaplastic ossification may also contribute to the variety in patterns that occur in chondromyxoid fibroma
Fig. 10.9
Occasionally, chondromyxoid fibroma lacks any lobularity; such cases are characterized by a diffuse proliferation of stellate-shaped cells in a loose myxoid background
Fig. 10.10
Low power view of chondromyxoid fibroma to show the spread into the cancellous jaw bone and the partial destruction of the root of the tooth in the tumor area. This condition is called external root resorption and usually occurs when the tumor grows slowly
Fig. 10.11
Chondromyxoid fibroma causes cortical expansion and remodeling but there is no perforation with subsequent spread into the overlying soft tissues
The clinically most relevant histologic differential diagnosis is with chondrosarcoma that may also have a lobulated growth pattern, myxoid matrix, and spindling of the nuclei. However, chondromyxoid fibromas typically contain cells with small, oval- to spindle-shaped nuclei without atypia whereas the nuclei in chondrosarcomas are usually larger, hyperchromatic, and with some degree of atypia. In those cases of chondromyxoid fibroma that show some atypical features as mentioned above and illustrated in Figure 10.7, the lobularity of the lesion will be helpful in differentiating between both diagnostic possibilities. In chondromyxoid fibromas of the skull base, chordoma may be considered as an alternative diagnosis. Chordomas contain epitheloid cells arranged in nests and cords and with vacuolated cytoplasm. Moreover, the chordoma cells are positive with cytokeratin markers. For further details on chordoma, see Chap. 11.
Regarding treatment, jaw resection has been recommended for extensive lesions whereas smaller lesions may be treated by curettage only [2].
10.3 Chondroblastoma
Chondroblastoma is a benign, cartilage producing neoplasm. Less than 10 % of them occur in the maxillofacial skeleton, especially in the lateral part of the temporal bone [1, 3]. Due to this site, hearing loss may occur.
Chondroblastomas are composed of mononuclear cells and chondroid matrix (Fig. 10.12). The mononuclear cells have an oval-to elongated nucleus that may display a characteristic longitudinal groove. Sometimes these cells contain brown granular pigment (Fig. 10.13). Mitotic figures are usually present, but not numerous. Multinucleated giant cells are a common feature (Fig. 10.14). Chondroid matrix varies in amount. Approximately one third of chondroblastomas exhibit calcification, usually occurs in a chickenwire-like pattern (Fig. 10.15). Secondary aneurysmal bone cyst formation may occur in one third of cases (Fig. 10.16) [1].
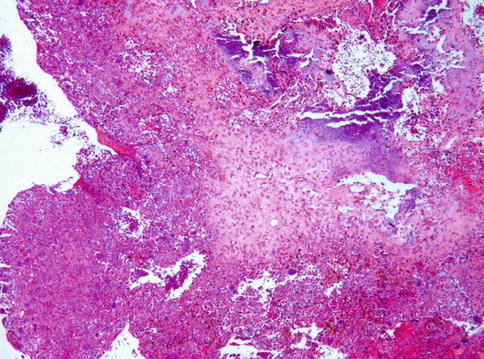
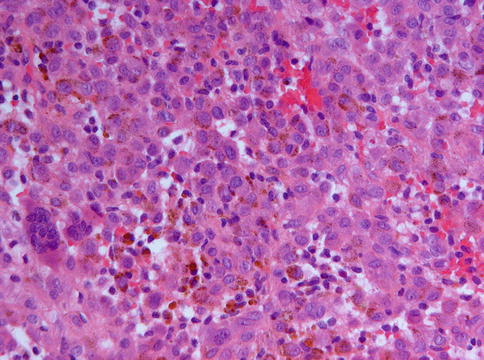
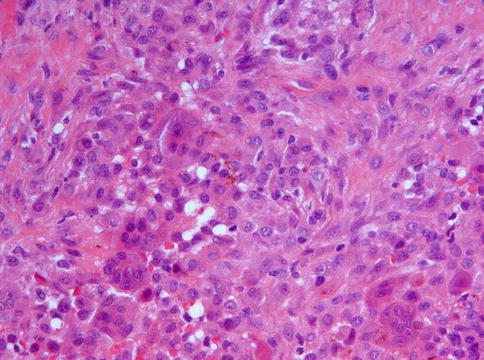
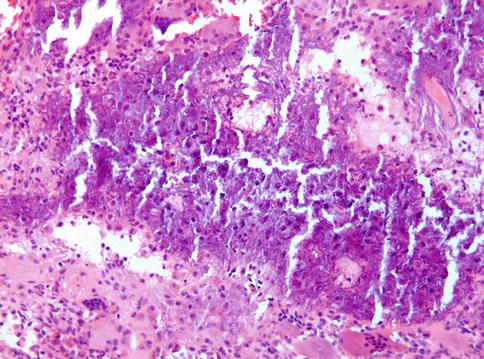
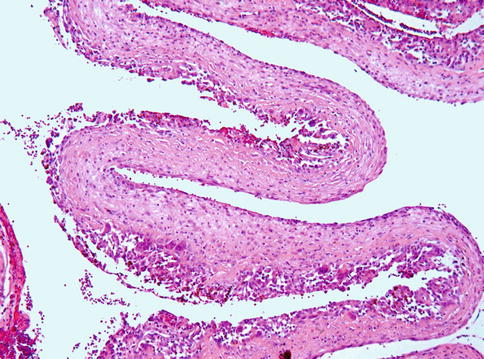
Fig. 10.12
Low power view of chondroblastoma to illustrate highly cellular tumor tissue with less cellular areas of chondroid matrix
Fig. 10.13
High power view to show the cellular component of chondroblastoma that is composed of mononuclear cells having an oval-to elongated nucleus that may display a characteristic longitudinal groove. Some of these cells contain brown granular pigment
Fig. 10.14
Multinucleated giant cells may form a major component of chondroblastoma
Fig. 10.15
Chondroblastoma with typical chickenwire calcification pattern
Fig. 10.16




Aneurysmal bone cyst component in chondroblastoma
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
