Table 4.1 Thyroiditis Classification by Inflammatory Response and Clinical Course | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
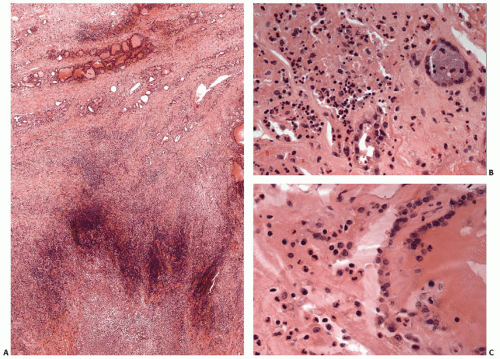 FIGURE 4.1. Acute thyroiditis secondary to a bacterial infection that initially affected extrathyroidal tissues. A: Low-power photomicrograph showing abscess (lower) with extension of inflammatory process into thyroid (upper). B and C: Medium- and high-power photomicrographs showing abundant neutrophils associated with damaged and necrotic follicles. |
protein and erythrocyte sedimentation rate are usually elevated.62 A minority of patients have significant elevation of antibodies to thyroglobulin (Tg) or thyroperoxidase (TPO), but these elevated titers are usually transient.58,59,63,64,65
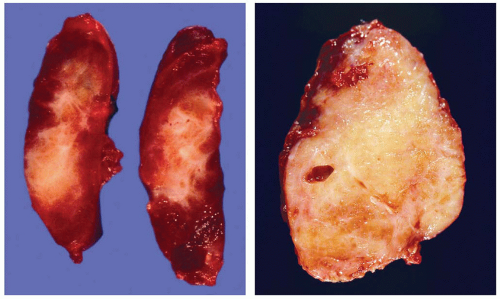 FIGURE 4.2. Cut surfaces of two different thyroids with subacute granulomatous thyroiditis. The inflammation and fibrosis in the thyroid pictured on the left resulted in a lesion clinically interpreted as a nodule. |
degenerated follicular cells.82,83,87 Oncocytic follicular cells are absent. In the latter stages, characteristic findings include multinucleated giant cells, strands of fibrous tissue, and a mixture of lymphocytes, macrophages, and possibly neutrophils.88,89,90 Follicular cells are usually scant to absent, and granulomata are rarely seen.
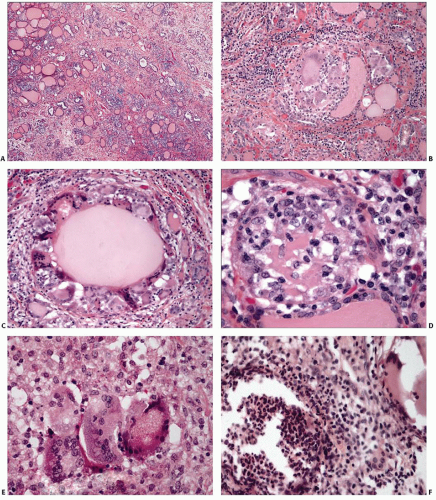 FIGURE 4.3. Subacute granulomatous thyroiditis. A: Low-power view showing decreased numbers of follicles. B and C: Medium-power views showing follicular damage with loss of epithelium and colloid and encirclement of follicle by multinucleated giant cells. D and E: High-power views showing granulomatous inflammation with predominance of macrophages and giant cells. F: High-power view showing mixture of acute and chronic inflammation with abundant neutrophils within an effaced follicle. |
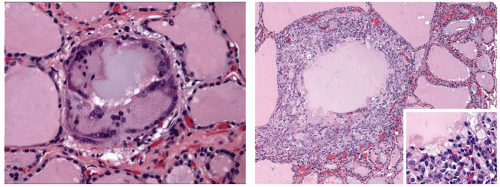 FIGURE 4.4. Palpation thyroiditis. Isolated follicle containing multinucleated giant cells (left). Disruption of a single follicle with a more intense surrounding inflammatory response (right). The high-power insert shows the predominance of macrophages. |
diseases has been observed.110,111,112,113,114 The most frequent coexisting disease is chronic lymphocytic (Hashimoto) thyroiditis. Although several cases of sarcoidosis with clinically overt chronic lymphocytic thyroiditis are relatively low, the incidence seems higher than by simple coincidence. The frequency of autoantibodies to Tg and/or TPO among individuals with sarcoidosis has been found to be as high114 as 27%. Rare cases of sarcoidosis associated with hyperthyroidism have also been reported.113,115,116,117
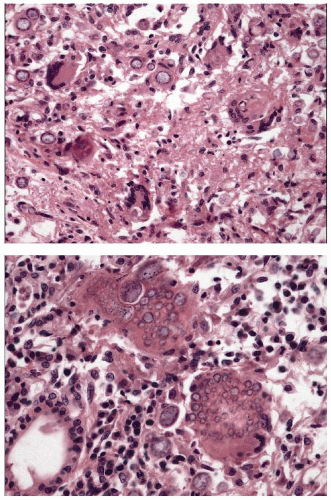 FIGURE 4.5. Coccidioidomycosis involving thyroid. An ill-defined granulomatous response is present focally (top) with scattered multinucleated giant cells. Overall, the inflammatory response in this case is predominately lymphoplasmacytic (bottom). Variably sized spherules are shown along with endospores within large spherules. |
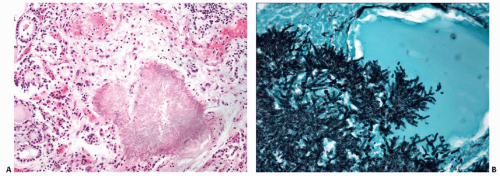 FIGURE 4.6. Fungal infection involving thyroid of an immunocompromised host. A: Medium-power photomicrograph showing aggregate of the fungus Scedosporium prolificans invading thyroid parenchyma with minimal inflammatory response (hematoxylin and eosin stain). B: High-power view showing fungal hyphae (Grocott methenamine silver stain). |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


