43 Thyroid and parathyroid disorders
Thyroid physiology
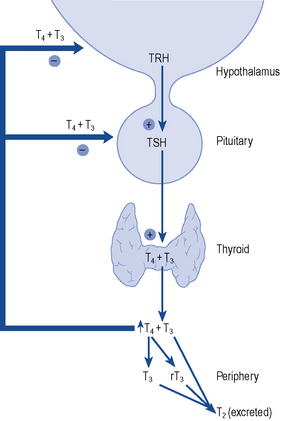
The thyroid gland consists of two lobes and is situated in the lower neck. The gland synthesises, stores and releases two major metabolically active hormones: Tetra-iodothyronine (Thyroxine, T4) and tri-iodothyronine (T3). Regulation of hormone synthesis is by variable secretion of the glycoprotein hormone TSH from the anterior pituitary. In turn, TSH is regulated by hypothalamic secretion of the tripeptide thyrotrophin-releasing hormone (TRH) (Fig. 43.1). Low circulating levels of thyroid hormones initiate the release of TSH and probably also TRH. Rising levels of TSH promote increased iodide trapping by the gland and a subsequent increase in thyroid hormone synthesis. The increase in circulating hormone levels feeds back on the pituitary and hypothalamus, shutting off TRH, TSH and further hormone synthesis.
Both T4 and T3 are produced within the follicular cells in the thyroid. The stages in synthesis are shown in Fig. 43.2. In summary:
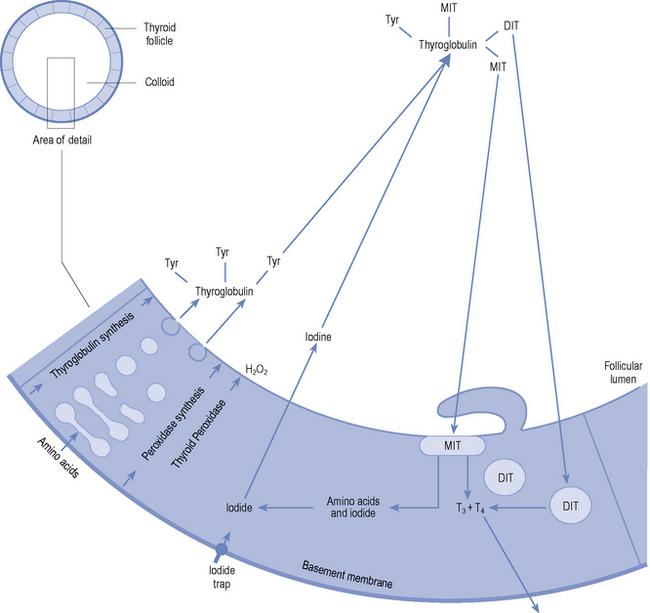
The ratio of T4:T3 secreted by the thyroid gland is approximately 10:1. Consequently, the gland secretes approximately 80–100 μcg of T4 and 10 μcg of T3 per day. However, only 10% of circulating T3 is derived from direct thyroidal secretion, the remaining 90% being produced by peripheral conversion from T4. T4 can therefore be considered a prohormone that is converted in the peripheral tissues (liver, kidney and brain) either to the active hormone T3 or to the biologically inactive reverse T3 (rT3). In the circulation, the hormones exist in both the active free and inactive protein-bound forms. T4 is 99.98% bound, with only 0.02% circulating free. T3 is slightly less protein bound (99.8%), resulting in a considerably higher circulating free fraction (0.2%). Details of protein binding are shown in Table 43.1.
Table 43.1 Plasma protein binding of thyroid hormones
| Carrier protein | Plasma concentration | Proportion of T4 and T3 bound (%) |
|---|---|---|
| Thyroid-binding globulin (TBG) | 15 mg/L | 75 |
| Transthyretin (formerly thyroid-binding prealbumin) | 250 mg/L | 10 |
| Albumin | 40 g/L | 15 |
Hypothyroidism
Aetiology
Primary hypothyroidism accounts for more than 95% of adult cases. It is usually due to a failure of the thyroid gland itself as a result of autoimmune destruction, or the effects of treatment of thyrotoxicosis. Hypothyroidism may be drug induced. Amiodarone and lithium cause hypothyroidism in around 10% of patients treated (see later). Secondary disease is due to hypopituitarism, and tertiary disease due to failure of the hypothalamus. Peripheral hypothyroidism is due to tissue insensitivity to the action of thyroid hormones. A more extensive classification is shown in Box 43.1.
Clinical manifestations
Hypothyroidism can affect multiple body systems, but symptoms are mainly non specific and gradual in onset (Box 43.2). Symptoms are frequently vague especially in the early stages. It is common for symptoms to be incorrectly attributed by patients and their relatives to increasing age. The reverse is also common in that patients who have read about, or have friends/family with, hypothyroidism will assume that it is responsible for symptoms of fatigue and weight gain. Thus, hypothyroidism is often confused with simple obesity and depression. Thyroid function tests give accurate diagnosis in all cases.
Box 43.2 Signs and symptoms of hypothyroidism
| Skin and appendages | Dry, cool, flaking, thickened skin |
| Reduced sweating | |
| Yellowish complexion. Puffy facies and eyes | |
| Sparse, coarse, dry hair | |
| Brittle nails | |
| Neuromuscular system | Slow speech |
| Poor memory and reduced cognitive function | |
| Somnolence | |
| Carpal tunnel syndrome | |
| Psychiatric disturbance | |
| Hearing loss | |
| Depression | |
| Muscle pain and weakness | |
| Delayed deep tendon reflexes | |
| Metabolic abnormalities | Raised total and LDL cholesterol |
| Macrocytic anaemia | |
| Gastro-intestinal | Weight gain with decreased appetite |
| Abdominal distension and ascites | |
| Constipation | |
| Cardiovascular | Reduced cardiac output |
| Bradycardia | |
| Cardiac enlargement |
Investigations
Testing thyroid function
As indicated earlier (and later in the section on thyrotoxicosis), a clinical assessment and measurement of free T4 and TSH are usually all that are necessary to arrive at an accurate diagnosis of thyroid state. All modern TSH assays now employ double antibody immunometric techniques, which are robust and highly reliable. Moreover, these assays are now so sensitive that they are able to identify thyrotoxic patients with TSH levels below the normal euthyroid range. Commercial free T4 and free T3 assays, however, are all indirect methods and are subject to interference from drugs and other disease states. As such, both T3 and T4 can be decreased as a non-specific consequence of systemic illness (‘sick euthyroid’ syndrome) and depression along with a host of drugs (Surks and Sievert, 1995), which can interfere with thyroid hormone metabolism and free hormone assays (Table 43.2). Such patients require specialist assessment and collaboration with the local laboratory to rule out confounding disease and pituitary failure.
Table 43.2 Drug effects on thyroid function
| Clinical/biochemical effects | |
|---|---|
| Decrease TSH secretion | |
| Dopamine | Hypothyroidism (rarely clinically important) |
| Glucocorticoids | |
| Octreotide | |
| Alter thyroid hormone secretion | |
| Iodide (amiodarone, contrast agents) | Both hyper- and hypothyroidism |
| Lithium | Hypothyroidism |
| Decrease T4 absorption | |
| Colestyramine/colestipol | Increased thyroxine dose requirement |
| Aluminium hydroxide | |
| Ferrous sulphate | |
| Calcium carbonate | |
| Multivitamins | |
| Sevelamer | |
| Protein pump inhibitors | |
| Sucralfate | |
| Alter T4 and T3 metabolism | |
| Increased hepatic metabolism | |
| Phenobarbital | Low T4 and T3 levels |
| Phenytoin | Normal or increased TSH |
| Rifampicin | |
| Carbamazepine | |
| Reduce conversion of T4 to T3 | |
| B-blockers | Lower T3 levels |
| Propylthiouracil | Normal or increased TSH |
| Amiodarone | |
| Glucocorticoids | |
| Reduce T4 and T3 binding | |
| Furosemide | Increased measured free T4 in some assays |
| Salicylates and NSAIDs | |
| Heparin | |
| Increase thyroglobulin levels | |
| Oestrogen and tamoxifen | Increased total T4 |
| Opiates and methadone | |
| Others | |
| Cytokines – interferon and interleukin 2 | Thyroiditis. Can produce hypothyroidism and thyrotoxicosis |
Treatment
The aims of treatment with thyroxine are to ensure that patients receive a dose that will restore well-being and that usually returns the TSH level to the lower end of the normal range (Vanderpump et al., 1996). All patients with symptomatic hypothyroidism require replacement therapy. T4 is usually the treatment of choice except in myxoedema coma where T3 may be used in the first instance. Before commencing T4 replacement, the diagnosis of glucocorticoid deficiency must be excluded to prevent precipitation of a hypoadrenal crisis. If in doubt, hydrocortisone replacement should be given concomitantly until cortisol deficiency is excluded.
It is important to avoid both under- and overtreatment. Hypothyroidism is very rarely life threatening, but adverse effects may result from prolonged overtreatment (which is indicated by a TSH level suppressed below the normal range). Though T4 exerts an effect on many organs and tissues, it is the effect on bone and the heart that give the greatest cause for concern. There is evidence that bone density is reduced in patients taking excessive T4 replacement therapy (Faber and Galloe, 1994; Uzzan et al., 1996), and that atrial fibrillation is more common if TSH is suppressed (Sawin et al., 1994). In order to minimise the risk of development of these complications, the dose of T4 should be carefully tailored to the needs of each individual patient. Some patients will have undetectable serum TSH levels while taking thyroxine and may complain of recurrent fatigue if the dose is reduced to permit the TSH to rise. In these patients, it may be permissible to leave the dose unchanged if levels of free T4 and T3 are normal, after a discussion of the relative risks and benefits with the patient (Vanderpump et al., 1996).
Patient care
Hypothyroidism requires lifelong treatment with T4. Patients on long-term drug therapy are recognised to have a low adherence with their medication regimen. Treatment with T4 is often terminated because patients feel well and think that treatment is no longer required. Patients should understand the effects of drug holidays on their health and thyroid function tests and should know that a normal TSH indicates adequate dosage. Written advice should be provided and monitoring of dosage should continue annually. There are a series of excellent patient information leaflets available on the British Thyroid Association website at www.british-thyroid-association.org
Despite adequate counselling, some patients persistently forget to take their tablets reliably, leading to variable thyroid state and wildly fluctuating test results. Other patients lack capacity to self-medicate reliably. There is evidence to show that weekly dosing with T4 is a safe and acceptable way to manage this type of patient, in whom family members or community staff can supervise treatment (Grebe et al., 1997; Rangan et al., 2007). There are no guidelines yet published, but in practice, patients are normally started on 500–700 μcg T4 weekly. Dose changes are made in exactly the same way by assessing TSH levels after 6 weeks of stable dosing.
Rarely, patients are seen in whom TSH levels fluctuate or remain elevated despite high doses of thyroxine and in whom adherence seems to be very good. There are a number of possible causes for this, including malabsorption of thyroxine which can be due to coeliac or inflammatory bowel disease or a number of commonly prescribed drugs (Table 43.2). Such patients will need a careful sequential assessment by an endocrine service (Morris, 2009).
Prevention
At present, nothing can be done to prevent autoimmune thyroid failure from developing; however, much can be done to ensure early detection and treatment. Careful follow-up of patients who have undergone radioiodine treatment, subtotal thyroidectomy or completed a course of treatment for thyrotoxicosis is essential along with monitoring of those prescribed amiodarone and lithium. An increase in TSH with normal concentrations of T3 and T4 will indicate the onset of hypothyroidism before the patient becomes symptomatic. Box 43.3 shows the prevalence of hypothyroidism after treatment for thyrotoxicosis.
Hyperthyroidism/thyrotoxicosis
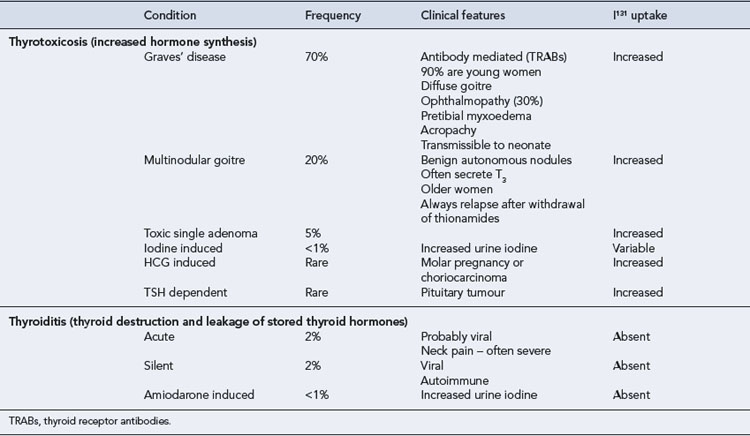
Hyperthyroidism is defined as the production by the thyroid gland of excessive amounts of thyroid hormones. Thyrotoxicosis refers to the clinical syndrome associated with prolonged exposure to elevated levels of thyroid hormone. This distinction is important when evaluating thyroid function tests (Table 43.3).
Epidemiology
Hyperthyroidism is a common condition. It has been estimated that there are 4.7/1000 women with active disease. When previously treated cases were included, the population prevalence rose to 20/1000 in women. As for hypothyroidism, it is much less common in men who have a lifetime prevalence of around 2/1000 (Tunbridge et al., 1977).



