Chapter 8 The Thyroid
A. Generalities

The thyroid may not be the most important organ in a busy general practice, but in physical diagnosis it is second only to the heart in number of examination errors and lack of physician’s confidence. This is unfortunate, since better skills may guide a more intelligent use of costly scans and better assessment of the likelihood of hyperthyroidism in anxious young patients.
B. Anatomic Review And Thyroid Gland Inspection
1 What are the thyroid’s landmarks?
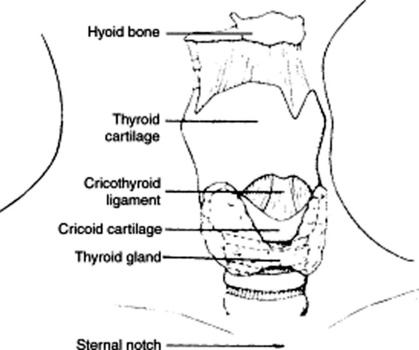
They are the laryngeal prominence and cricoid cartilage. Start your exam by identifying the hyoid bone, a horseshoe mobile structure just under the mandible, so called because of its “upsilon” like shape. Immediately below it, you will find the thyroid cartilage, which can be readily identified by its V shape, the midline notch on the superior edge (laryngeal prominence), and its being the most prominent structure in the anterior neck (Adam’s apple). Just below it, separated by a little gap (the cricothyroid recess), is the horizontal ring of the cricoid cartilage. The thyroid isthmus lies immediately below, 4 cm from the laryngeal prominence. It connects the two lateral lobes of the gland by crossing the trachea over the second, third, and sometimes even the fourth ring. Note that while the distance between isthmus and landmarks (cricoid cartilage and laryngeal prominence) is constant in all individuals, the distance between laryngeal prominence and suprasternal notch is variable. This may result in glands that are either low lying or high lying in the neck (see Fig. 8-1).
2 Where are the thyroid lobes in relation to other neck structures?
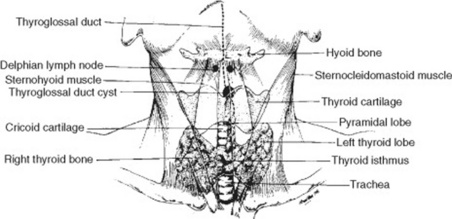
The lateral lobes fan out from the midline isthmus just below the cricoid cartilage, curve posteriorly around the sides of trachea and esophagus, and then ascend backwards and upward like the two branches of a V (Fig. 8-2). Each lobe is 3–5 cm long, so that the lower margin reaches down to 2 cm above the clavicle (and fifth to sixth tracheal ring), whereas the upper margin extends instead upward to the middle of the thyroid cartilage. Except for its isthmus, the thyroid is covered by thin, strap-like muscles, of which only the sternocleidomastoid muscles (SCMs) are visible. Since the fascial envelope of the gland is continuous with the pretracheal fascia of both the hyoid and cricoid, the isthmus will ascend and descend with the larynx upon swallowing. This is important because it helps in distinguishing the thyroid from other neck structures.
4 What is the best way to Inspect the thyroid?
 It raises the trachea further up from the suprasternal notch, thus moving upward any low-lying thyroid, too.
It raises the trachea further up from the suprasternal notch, thus moving upward any low-lying thyroid, too.

Once the patient is well positioned, inspect the midline, 2–3 cm above the clavicles. Look within the SCMs for the inferior margins of the thyroid lobes, and then locate the isthmus (just below the cricoid cartilage). Finally, inspect the superior margins of the lobes (which should barely touch the sides of the thyroid cartilage). Look also for any possible pyramidal lobe. Use cross-illumination with a penlight to better accentuate shadows and nodules. Observing the gland from the side also may help detect possible protrusions. Note that unless a goiter is present, there should be no bulging between cricoid cartilage and suprasternal notch. Hence, a goiter is effectively ruled out if the gland is not visible on lateral view of an extended neck. Once inspection is complete, assess the associated venous structures of the neck, and record any possible abnormality (Figs. 8-3 and 8-4).


5 How helpful is swallowing during inspection or palpation?




C. Thyroid Gland Palpation
13 How do you palpate a thyroid?
 Start with proper positioning. In contrast to inspection, a slight ipsilateral flexion and rotation of the neck may allow you easier access to a mass, nodule, or gland asymmetry. Hence, to palpate the right lobe, ask the patient to flex and rotate the neck toward the right. Do the opposite for the left lobe. Yet, as for inspection, a slight neck extension (10 degrees) may help, too, by lifting the top of a substernal goiter into a more accessible position. Still, most experts recommend flexion over extension. Finally, ask the patient to swallow repeatedly while you palpate the moving gland.
Start with proper positioning. In contrast to inspection, a slight ipsilateral flexion and rotation of the neck may allow you easier access to a mass, nodule, or gland asymmetry. Hence, to palpate the right lobe, ask the patient to flex and rotate the neck toward the right. Do the opposite for the left lobe. Yet, as for inspection, a slight neck extension (10 degrees) may help, too, by lifting the top of a substernal goiter into a more accessible position. Still, most experts recommend flexion over extension. Finally, ask the patient to swallow repeatedly while you palpate the moving gland.
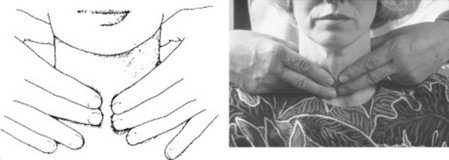
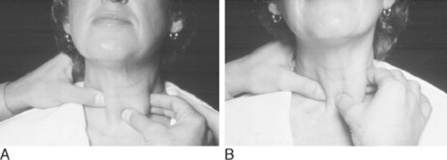
 The posterior bimanual approach is the most commonly used. While standing behind the patient, place the index and middle fingers of both hands along the midline of the neck, just below the chin. These should be 2 cm above the suprasternal notch, and 0.5 cm inside the medial margin of the SCM. From that position, locate first the thyroid cartilage, then slide gently down to the horizontal groove that separates it from the cricoid cartilage. This is covered by the cricothyroid membrane, which overlies the first tracheal ring and represents the reference point for emergency tracheostomy (cricothyroidotomy) in upper airway obstruction. Continue sliding down until you reach the next well-defined tracheal ring. At this point, you are on the thyroid isthmus, which lies between the cricoid cartilage and suprasternal notch, and is almost never palpable. Slide your fingers laterally on the isthmus, and go around for approximately 2–3 cm along each side: you will be touching the two main lobes of the gland. Use a soft touch to minimize discomfort and maximize yield. If the gland is enlarged, evaluate its consistency. Then ask yourself whether the enlargement is asymmetric or bilateral, nodular or diffuse, with movable overlying layers associated with adenopathy. Use one hand to fix the trachea and the other to palpate one lobe at a time (Figs. 8-5 and 8-6). You can practice by placing the second and third fingers of both hands over your own sternal notch. Move them up 2 cm above the clavicles (toward the lower thyroid poles), then palpate each lobe in detail.
The posterior bimanual approach is the most commonly used. While standing behind the patient, place the index and middle fingers of both hands along the midline of the neck, just below the chin. These should be 2 cm above the suprasternal notch, and 0.5 cm inside the medial margin of the SCM. From that position, locate first the thyroid cartilage, then slide gently down to the horizontal groove that separates it from the cricoid cartilage. This is covered by the cricothyroid membrane, which overlies the first tracheal ring and represents the reference point for emergency tracheostomy (cricothyroidotomy) in upper airway obstruction. Continue sliding down until you reach the next well-defined tracheal ring. At this point, you are on the thyroid isthmus, which lies between the cricoid cartilage and suprasternal notch, and is almost never palpable. Slide your fingers laterally on the isthmus, and go around for approximately 2–3 cm along each side: you will be touching the two main lobes of the gland. Use a soft touch to minimize discomfort and maximize yield. If the gland is enlarged, evaluate its consistency. Then ask yourself whether the enlargement is asymmetric or bilateral, nodular or diffuse, with movable overlying layers associated with adenopathy. Use one hand to fix the trachea and the other to palpate one lobe at a time (Figs. 8-5 and 8-6). You can practice by placing the second and third fingers of both hands over your own sternal notch. Move them up 2 cm above the clavicles (toward the lower thyroid poles), then palpate each lobe in detail.
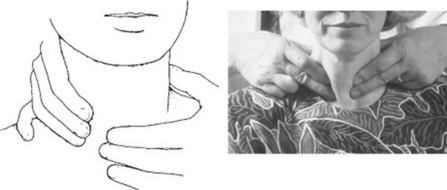
 The anterior single-hand approach. Face the patient and use the thumb plus the index finger of one hand to palpate each lobe. Do this just inside the SCMs (Fig. 8-7).
The anterior single-hand approach. Face the patient and use the thumb plus the index finger of one hand to palpate each lobe. Do this just inside the SCMs (Fig. 8-7).
14 What are the normal variants in size and location?
 Women have larger and more easily palpable glands.
Women have larger and more easily palpable glands.
 In 1% of the population, the entire left lobe (or its lower half) is absent.
In 1% of the population, the entire left lobe (or its lower half) is absent.
 The right lobe is often larger than the left.
The right lobe is often larger than the left.

 Posterior, extracapsular, and ectopic tissue can occur in 5% of normal glands. This usually extends from the posterior aspect of the tongue toward the pyramidal lobe, and occasionally down into the mediastinum (see Chapter 6, Nose and Mouth, question 103).
Posterior, extracapsular, and ectopic tissue can occur in 5% of normal glands. This usually extends from the posterior aspect of the tongue toward the pyramidal lobe, and occasionally down into the mediastinum (see Chapter 6, Nose and Mouth, question 103).
D. Additional Components Of The Focused Thyroid Examination






17 What are the potential complications of a large goiter?
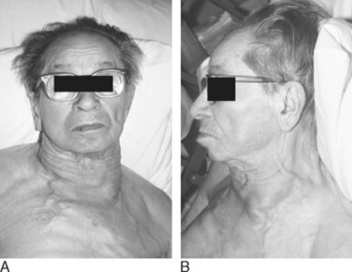
Mostly obstructive, with impaired venous return (facial plethora) and a compression of the esophagus and trachea that may result in dysphagia and dyspnea. Stridor occurs in 10% of substernal goiters; tracheal deviation in one third. Although Graves’ glands may be up to two times normal (i.e., 40 gm), multinodular goiters are usually the most prominent offenders. When a large mediastinal or substernal thyroid obstructs the superior vena cava, there will be venous engorgement over the anterior chest and neck and possible impairment of cerebral venous return (Fig. 8-8). If reversible, all these findings can be unmasked by the Pemberton’s maneuver.
18 What is the Pemberton’s maneuver?
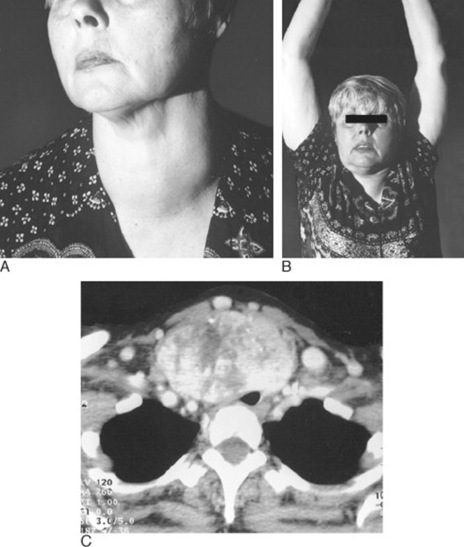
A reversible superior vena cava (SVC) obstruction caused by a substernal goiter being “lifted” into the thoracic inlet as a result of arm raising. This makes the goiter behave like a “thyroid cork,” blocking the inlet and thus preventing venous return. To carry out the maneuver, ask the patient to elevate the arms above the level of the head, as if surrendering (“elevat[ing] both arms until they touch the sides of the head,” in Pemberton’s words). If the sign is present, “after a minute or so, congestion of the face, some cyanosis, and lastly distress become apparent.” In fact, the test is considered positive when the patient experiences either facial plethora (blue or pink suffusion of the neck and/or face due to venous stasis) or head congestion, dizziness, and stuffiness. If severe, the “thyroid cork” may even cause dyspnea and hypotension. The test is negative if nothing happens after 3 minutes of arm elevation (Fig. 8-9).
19 What is the significance of a positive Pemberton’s maneuver?



23 How do you distinguish a thyroid bruit from other neck sounds?
 A venous hum is heard lower in the neck than a thyroid bruit. It is also suppressed by compression of the ipsilateral neck veins. Note that the continuous character of a “hum” cannot reliably differentiate it from a bruit, since 20–36% of all hyperthyroid patients have indeed a continuous bruit (due to arteriovenous communications within the hyperplastic gland). Compression of neck veins will help differentiate the two.
A venous hum is heard lower in the neck than a thyroid bruit. It is also suppressed by compression of the ipsilateral neck veins. Note that the continuous character of a “hum” cannot reliably differentiate it from a bruit, since 20–36% of all hyperthyroid patients have indeed a continuous bruit (due to arteriovenous communications within the hyperplastic gland). Compression of neck veins will help differentiate the two.
 A carotid bruit is heard higher and lateral to the gland than a thyroid bruit.
A carotid bruit is heard higher and lateral to the gland than a thyroid bruit.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


