Robert L. DuPont, MD, Bruce A. Goldberger, PhD, F-ABFT, and Mark S. Gold, MD, FASAM
112
EVOLUTION OF DRUG TESTING
Over the past five decades, drug testing technology has progressed rapidly, permitting the identification of drugs and their metabolites at far lower concentrations, far more economically, due to the development of benchtop mass spectrometry. At the same time, drug testing expanded beyond urine to include testing of oral fluid (saliva), hair, and sweat. The most controversial issue regarding drug testing—the problem of false positives—has been virtually eliminated.
When drug testing migrated from clinical settings to prevention in the workplace, controversy ensued over the application of modern drug testing technology, and the use of forensic standards became commonplace for the first time in toxicology. Drug testing also is used in research and evaluation studies to validate self-report surveys of drug use and to evaluate the effectiveness of treatment programs in reducing patients’ drug use.
Drug testing is now expanding throughout medical practice following the lead of pain management clinics and other settings where potent opioids and other medications are prescribed on a regularly basis. Drug test profiles are extensive and include many opioids and benzodiazepines, as well as illicit drugs (including amphetamines, cannabinoids—metabolites of cannabis—and cocaine). These analyses are used to monitor patient adherence to prescribed medications and to identify the potential use and abuse of other, nonprescribed substances.
THE SCIENCE OF DRUG TESTING
Although drugs of abuse, including alcohol, are ingested through many routes of administration (e.g., oral, intranasal, smoking, and intravenous), these are distributed by the blood to all areas of the body. For this reason, drugs and their metabolites can be detected in nearly all body fluids and tissues.
In general, drugs and drug metabolites are detectible in urine for 1 to 3 days after acute administration, although following heavy chronic use, some drugs—especially cannabis—may be detected for longer periods of time. After a single episode of cannabis use, many users have negative urine tests at usual cannabinoid cutoffs within 24 hours, and almost all will be negative within 3 to 5 days of last use. However, with chronic use of cannabis, positive urine tests can be obtained for a month or longer.
In the most common drug testing programs, an initial immunoassay screening test is followed by a more sensitive and specific confirmation test that is based on mass spectrometry. The confirmation of drugs and drug metabolites by gas chromatography–mass spectrometry (GC-MS) is now compulsory in forensic settings and when there are serious consequences for a positive test. However, in many clinical settings (such as emergency departments, drug treatment programs, and the criminal justice system), only the initial immunoassay test is required, thereby reducing the cost of testing and increasing the speed with which results are available.
The GC-MS technique identifies drugs and drug metabolites primarily on the basis of the chemical structure of the compound. It is a highly accurate method of detecting drugs and drug metabolites; the false-positive rate of GC-MS is nil.
The current highest analytical standard is liquid chromatography–mass spectrometry–mass spectrometry (LC-MS/MS), which is a sophisticated technology that is increasingly being used, particularly in the field of pain management. LC-MS/MS technology can identify hundreds of different analytes in a single sample.
ON-SITE VERSUS LABORATORY ANALYSIS
Most drug tests are conducted at clinical laboratories following the collection of a sample at some other site (e.g., at a drug treatment center or a physician’s office). The laboratory testing process usually requires a day or two from the time of collection until the result is available to the clinician. However, in recent years, more drug testing is done on-site when the initial immunoassay test is done at the point of collection rather than at a laboratory. In forensic settings, the sample that tests positive on-site is sent to a laboratory for a confirming test before being reported as positive.
The ability to obtain results at the time of collection is enormously useful. However, on-site tests, especially oral fluid tests, may be less sensitive than are laboratory-based analyses. In addition, a confirmation test is not available on-site. On-site tests seldom produce false- positive results, although that does happen. False-negative results are more common when using on-site test kits, and this problem mitigates some of the benefits of immediate results.
CHOICE OF MATRIX
The choice of a testing matrix relates to the period of time after drug use that the drugs and their metabolites are detectable, the distribution of the drugs and drug metabolites, the ease of specimen collection, and the level of vulnerability to cheating.
Urine is a particularly attractive matrix for drug testing because it is easy to collect, most drugs and drug metabolites can be readily detected in urine without complex extraction processes, and drugs and their metabolites often can be detected for longer periods of time in urine than in other biologic fluids. Nevertheless, testing for drugs of abuse in oral fluid, hair, and sweat is valuable.
Urine
Virtually all clinical laboratories perform drug tests on urine samples, creating a highly competitive marketplace whose effect is to lower costs and enhance the choice of drug test suppliers. Because urine testing is dominant in the drug testing marketplace, it is relatively easy and inexpensive to add drugs to the federal government’s basic five-drug panel, which consists of cannabis, cocaine, phencyclidine (PCP), amphetamines, and opiates. This is a major advantage of urine testing, as a large proportion of drug use involves drugs other than those in the basic panel. Widely referred to as the “DHHS-5” (formerly “NIDA-5”) because the Department of Health and Human Services manages the standards for federally regulated drug testing, in 2010, confirmatory testing of the panel was expanded by DHHS to include the following amphetamines: methylenedioxymethamphetamine, methylenedioxyamphetamine, and methylenedioxyethylamphetamine. Urine drug test suppliers offer more extensive panels of commonly used drugs and can add additional drugs when needed.
Urine is especially vulnerable to cheating, with an expanding range of techniques actively promoted on the Internet.
Hair
Drugs and drug metabolites are incorporated in the hair while it is formed in the hair follicle. Head hair grows approximately one-half inch a month. The typical hair specimen is at least 1.5 inches long, thus producing a record of drug use over the preceding 90 days. However, it takes about 1 week for hair to grow from the base of the follicle to a point at which it can be snipped at the level of the scalp. Therefore, there is no record in hair of drug use during the week prior to sample collection. Alcohol is not incorporated in hair, although alcohol’s major metabolites, including ethyl glucuronide (EtG), are detectable in hair samples.
Over the course of the 90 days covered by a typical 1.5-inch hair sample, even a few uses of most drugs of abuse are detectable. Cannabis is an exception because concentrations of tetrahydrocannabinol (THC) and cannabinoids in the body—including the hair—are significantly lower than the concentrations of most other drugs of abuse. For this reason, cannabis must be used repeatedly for the entire 90 days to produce a positive result at the standard cutoff concentrations. Hair tests are very resistant to cheating because hair collection is always under direct observation.
Hair testing has been criticized as racially biased because of an early study finding that when a mouse was given an antipsychotic drug, higher concentrations of the drug were found in the black hair on that mouse than in the white hair. More recently, several studies using large samples of tested subjects unanimously found that the proportion of subjects who tested positive is the same for African Americans and Whites, based on urine testing, hair testing, and self-report.
Oral Fluid
Saliva or oral fluid can be analyzed for drugs of abuse with both on-site and laboratory-based techniques. Oral fluid testing is highly resistant to cheating, as the oral fluid sample is collected under direct observation. The most significant problem with oral fluid testing is that the tests are less sensitive to cannabis use, although the detection of other drugs of abuse is roughly similar for oral fluid testing and urine testing. In general, oral fluid is most closely correlated with blood testing, with which saliva is in equilibrium. This means that oral fluid testing generally identifies drug use within the 12 to 24 hours prior to sample collection.
The on-site kits for oral fluid testing are particularly prone to miss cannabis use because the assay is generally less sensitive than are laboratory-based analyses. As the tests are refined to have greater sensitivity, this limitation of both hair and oral fluid testing can be expected to vanish. For many applications, oral fluid testing is widely expected to be the test of the future because it does not pose the problems with direct observation of sample collection that occurs with urine, making it resistant to cheating.
Sweat
A patch that is similar to a nicotine patch worn in smoking cessation is applied to the tested person and is removed after a week or two for analysis at a laboratory. The sweat is collected in an absorbent pad that is protected by a permeable cover. The water in sweat evaporates through the covering membrane, leaving the drug and drug metabolites concentrated in the gauze.
Sweat allows prospective testing from the time the patch is applied, whereas all other drug tests are retrospective from the time of collection. There is no on-site option for the analysis of drugs and drug metabolites in sweat. Sweat testing is resistant to cheating because the patch puckers when removed and reapplied.
Breath
Alcohol is easily quantified in breath, with the results widely used in clinical and medicolegal settings. In addition, recent studies have demonstrated the presence of amphetamines, cocaine, opiates, and THC. Breath testing for alcohol has become an important tool to detect impaired driving. It has the advantages of being resistant to cheating and far easier to collect than urine, oral fluid, or hair. As the test technology for drugs improves, including the development of an improved collection device, it is likely that drugs of abuse will be detected in breath as these now are for alcohol.
Testing for Alcohol
Since the dose of alcohol needed to produce brain reward is a thousand or more times higher than the dose of the commonly used drugs of abuse, testing for drugs has been more challenging and more reliant on the evolution of technology than it has been for alcohol.
Alcohol is rapidly metabolized, primarily by the liver, so alcohol concentrations in the blood decrease rapidly—typically to zero within a few hours after the last drink. The acute impairing effects of alcohol are related to the blood alcohol concentrations as modified by the moderating effects of tolerance and the subject’s familiarity with the task being measured. The alcohol concentration is in equilibrium with the blood at the time the urine leaves the kidneys. The urine in the bladder is a reflection of the blood alcohol concentrations over the period of time that the urine in the bladder was being produced by the kidneys. For this reason, the urine alcohol concentration lags the blood alcohol concentration at the time of urination, meaning that the urine alcohol concentration is lower than the blood alcohol concentration at the time of urine collection during the ascending slope of the blood concentration and higher during the descending slope of blood concentration after drinking stops. The detection window for urine alcohol tests generally is 12 hours or less after drinking has stopped, in contrast to 1 to 3 days for detection of most drugs of abuse.
An important new testing option is the test for EtG or ethyl sulfate, both of which are metabolites of alcohol that are found in urine for 5 to 7 days following the consumption of alcohol. These tests are especially useful in settings where alcohol use is completely prohibited. A negative EtG test is especially valuable in helping to establish that the donor of the urine sample has not used alcohol in the preceding 5 to 7 days. Because the EtG tests may be positive when the donor has used an alcohol hand sanitizer or an alcohol-containing mouthwash, interpreting a positive EtG test result requires clinical judgment, especially if the consequences for a single positive test are severe. Individuals who are subject to EtG testing for alcohol should be warned specifically and in detail to avoid alcohol-containing products or risk a positive test result.
Comparing Matrices
Refer to Table 112-1 for a comparison of the clinically available test matrices. There are clinical settings in which each of the matrices discussed in this chapter is particularly useful. Urine is the default matrix for most drug tests because it is the most familiar and because most clinical laboratories conduct these tests. Urine also is the most practical matrix when special-order tests are required, including tests for drugs that are less commonly used. On the other hand, urine has a much shorter detection window than does hair. In addition, urine is the matrix most vulnerable to cheating. Oral fluid is the most easily obtained matrix, but can be less sensitive to drug use and have a shorter detection window than urine. Sweat patch testing is prospective—meaning it identifies drug use after the patch is in place. Like oral fluid and hair testing, sweat patch testing is highly resistant to cheating. Hair testing is particularly helpful in scheduled testing, including preemployment tests where cheating is common. On the other hand, hair is the most expensive drug test matrix.
TABLE 112-1. COMPARISON OF BLOOD, URINE, HAIR, ORAL FLUID, AND SWEAT PATCH TESTING FOR DRUGS OF ABUSE
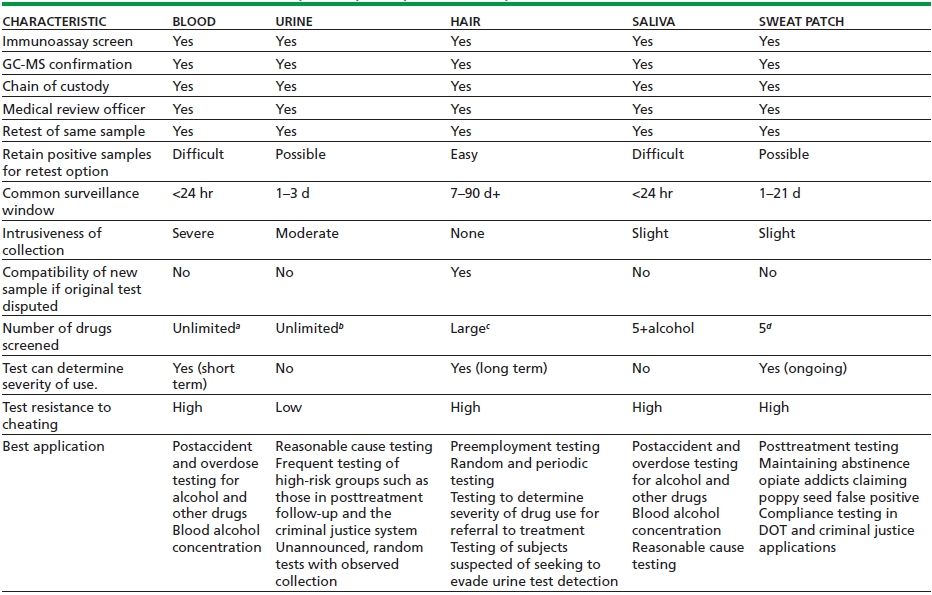
aBlood testing for alcohol is routine, but blood testing for drugs is done by only a few clinical laboratories in the United States.
bUrine tests for nonroutine drugs are available from most reference laboratories.
cHair testing is commonly performed for the “NIDA-5” (cocaine, opiates, marijuana, amphetamines, and PCP). However, a large number of drugs and metabolites can be detected, and routine broad testing is performed in several toxicology reference laboratories.
dCommonly limited to the “NIDA-5.” Tests can also be performed for alcohol.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


