abdominal cavity simultaneously. After descent, the abdominal opening of the canal closes. The scrotum sits dorsal to the penis, the male sexual organ and the male structure for urination. Because of their location outside the body, the testes remain at a lower-than-body temperature. This provides optimal conditions for spermatogenesis, or sperm formation.
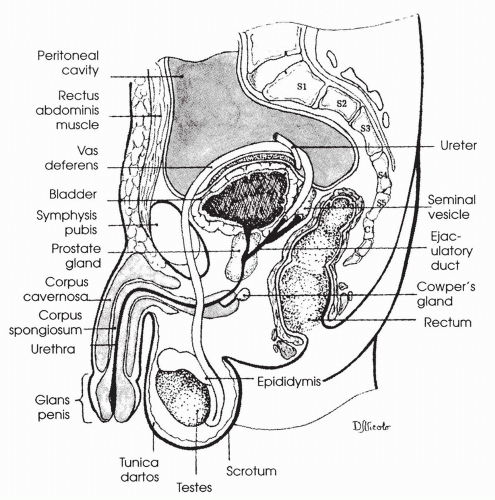 FIGURE 20-1 Side view of male genitourinary anatomy. (From Bullock, B. L. & Rosendahl, P. P. (1992). Pathophysiology: Adaptations and alterations in function (3rd ed.). Philadelphia, PA: Lippincott Williams & Wilkins.) |
nerves exit the spine from the upper lumbar areas and innervate the smooth muscle of the vas deferens and ampulla. Sympathetic fibers release the neurotransmitter norepinephrine, which causes smooth muscle contraction. Sympathetic fibers also innervate and cause contraction of the prostate and the seminal vesicles. Descending neurons from higher centers of the brain, including the cerebral cortex, influence the firing of the parasympathetic and sympathetic fibers.
further activation of the sympathetic fibers and smooth muscle contraction of the ducts. Motor neurons to skeletal muscles at the base of the penis are also activated, leading to contraction of these muscles. The culminating responses are wavelike, rhythmic contractions associated with intense pleasure. During these contractions, semen is forcefully propelled through the urethra and out of the urethral opening. Emission and ejaculation comprise the male orgasm. Heart rate and respiratory rate reach a maximum at this time.
the tubule, and again through the activation of a cAMP second messenger system, stimulates the synthesis of the steroid hormone testosterone. Testosterone diffuses into the seminiferous tubules and binds to the Sertoli cells, stimulating them to continue to secrete the proteins, ions, and nutrients required to maintain proliferation and differentiation of the sperm. One protein that is manufactured by the Sertoli cells, androgen-binding protein, ensures that levels of testosterone remain high in the lumen of the seminiferous tubule. Mature Leydig cells usually develop at approximately 10 years of age in a boy.
Increased protein anabolism and muscle mass.
Increased bone growth and strength.
Male pattern of hair on the face, axillary, and pubic regions. Hair growth is thick on most areas of the body.
Increased metabolic rate, probably as a result of increased protein anabolism (buildup) and muscle mass formation. Increased metabolic rate raises the caloric needs of males, beginning at puberty, compared to females.
Proliferation and activation of sebaceous glands in the skin, which produce an oily substance called sebum. Increased amounts of sebum can cause acne, especially during teenage years.
A deepening voice, as a result of hypertrophy of the larynx.
Male pattern baldness, typically beginning with a bald spot on the top of the head. A genetic tendency influences male pattern baldness.
TABLE 20-1 Summary of Male Reproductive Organ Alterations | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Increased frequency of urination, with delay in initiating urination and a reduction in the force of the urine stream.
Decreased diameter of the urinary stream.
As the condition progresses, the bladder may not empty completely, causing dribbling or urine overflow. The time required to void increases.
Diagnosis involves a good history and physical examination coupled with the use of imaging techniques. Biopsy of the prostate may be required to rule out neoplasia.
With advanced BPH, urinary tract obstruction may occur as urine is unable to pass through the prostate. Urinary obstruction can lead to urinary tract infections and, if unrelieved, renal failure.
Mild prostate enlargement may not be treated, but followed in a “wait and see” manner.
Active surveillance involves annual monitoring for disease progression including a history, physical examination, and symptom score.
With more significant enlargement, medical therapy will be initiated. Alphablockers antagonize alpha-adrenergic receptors in the smooth muscle of the prostate causing relaxation of the muscle fibers thereby decreasing tension in
the prostate. 5-alpha reductase inhibitors block the conversion of testosterone to dihydrotestosterone causing the prostate to shrink in size. A combination of the two types of medications significantly increases symptom improvement as opposed to monotherapy.
Surgical approaches that involve minimal invasiveness include transurethral incision of the prostate (TUIP). In this procedure, the gland is split in half surgically to reduce pressure on the urethra. Lasers may be used to split the prostate.
Other minimally invasive procedures to reduce the size of the prostate include transurethral needle ablation, transurethral vaporization, and transurethral microwave therapy.
If obstruction to urine flow is severe, transurethral prostatectomy (TURP) may be required to remove the enlarged prostate. Complications may include ED and incontinence.
A permanent catheter might be placed in patients unwilling to undergo or unable to tolerate surgery.
Annual digital rectal examinations and screening for prostate-specific antigen (PSA) are encouraged to identify a malignancy that may arise from hyperplastic cells.
Urethritis may present with pain and burning on urination. A discharge from the penis may be present.
Epididymitis may present with acute scrotal or inguinal pain. Flank pain may be present. The scrotum may be inflamed and tender on the affected side.
Orchitis usually presents acutely with a very high fever (104°F) and swelling and redness of the testicle and scrotum. The individual appears very ill, and malaise is obvious.
Prostatitis from an ascending urinary tract infection usually presents with painful and frequent urination. Interrupted or slow urine stream and nocturia (urination at night) may be present. Fever and malaise are common. Low back or perineal pain is common, especially when standing. Digital examination reveals a very tender and enlarged prostate.
Diagnosis involves a thorough history and physical examination. Blood and urine cultures for the identification of an infectious organism may be required.
Epididymitis and orchitis may cause infertility, related to poor testicular blood flow, and infarct of the testicular cells.
Antibiotic therapy is required for all bacterial or chlamydial infections.
Orchitis is treated with bed rest, analgesics for pain, and elevation of the testicles to increase venous drainage. Cold compresses may reduce initial inflammation. If a testicular abscess occurs, surgical removal of the testicle may be necessary.
cancer usually develops in men between 40 and 80 years of age and is more common in African Americans than in Caucasians. Secondary penile cancer may occur from metastasis of bladder, rectal, or prostate cancer.
Penile cancer is characterized by a painless wartlike growth or an ulcerative lesion under the prepuce. It may also be a reddened lesion with plaque.
Testicular cancer is characterized by the development of a mass in the testis, which may become painful as it grows. Testicular heaviness or aching may occur. Gynecomastia may develop.
Prostate cancer may be asymptomatic or associated with increased frequency and urgency of urination, and a decrease in the force of the urine stream. Blood may be passed in the ejaculate, and in advanced disease, back pain may be present.
Biopsy of cells of the penis can diagnose and stage penile cancer.
Transillumination of the testes, ultrasound, and MRI may identify a testicular mass and support clinical findings of a testicular cancer.
Tumor markers commonly associated with testicular cancer include alphafetoprotein (AFP), beta human chorionic gonadotropin (hCG), and lactate dehydrogenase (LDH).
A digital rectal examination (DRE) may reveal a fixed, firm mass in the prostate, suggestive of a tumor. The mass is often painless with irregular borders and results in asymmetry of the prostate gland. Ultrasound may be used to pinpoint the location of a prostate tumor. A biopsy of prostate cells taken via a transurethral resection can confirm the diagnosis of prostate cancer. DRE should be conducted annually beginning at 50 years of age.
Prostate-specific antigen (PSA), a blood test that measures the level of a glycoprotein released by the prostate gland, can be used to identify the presence of even early-stage prostate cancer. Current recommendations are to perform a biopsy if the PSA level is greater than 4 nanograms per milliliter (ng/mL) of blood; levels greater than 10 ng/mL suggest cancer. However, PSA elevation may occur with noncancerous conditions such as prostatitis or benign prostatic hyperplasia (BPH). Likewise, in approximately 25% of men, PSA measurements may be in the normal range even when cancer is present. The need to treat stage A cancers detected by PSA assay is controversial, especially in elderly men.
Measurement of PSA levels coupled with findings from a digital exam offer the most sensitive screening results. PSA levels should be drawn prior to the
digital exam to minimize the risk of a false-positive reading due to manipulation of the prostate.
Transrectal ultrasound can be used to view the prostate using sound waves.
Diagnosis is confirmed with a biopsy.
Untreated, progressive penile cancer has an extremely high mortality rate (about 90%).
Testicular cancer may metastasize to the lungs, lymph nodes, liver, bone, or central nervous system.
Survival with prostate cancer depends on the stage at diagnosis. Most men diagnosed with stage D cancer die within 3 to 5 years.
ED and incontinence may develop as a result of any of the male reproductive cancers or may develop following treatment of the cancers.
For penile cancer, treatment may range from excisional biopsy to a total penectomy. Radiation and chemotherapy may also be required.
For testicular cancer, surgery to remove the affected testis is performed. Radiation and chemotherapy are provided.
A chest radiograph and a lymph node biopsy are performed on men with testicular cancer to rule out metastasis.
Watchful waiting may be adequate for some elderly men with stage A prostate cancer.
Radical prostatectomy (surgical removal of the prostate) or radiation therapy is usually used to treat all stage B and C prostate tumors and all stage A tumors in young men. Treatment options can include proton-beam radiation, implanted radiation seeds, and cryotherapy. Stage D tumors are treated with hormonal therapy to slow the spread of the disease and palliative measures to reduce pain. Hormonal therapy includes antiandrogen drugs, estrogen therapy, and drugs that block the release of the hypothalamic GnRH (leuprolide). Orchiectomy (removal of the testes) may accompany hormonal therapy.
of an embryo and fetus until survival outside the womb is possible. Internal reproductive structures that allow a female to meet these roles include the ovaries, fallopian tubes, uterus, and vagina. After the birth of her infant, the female’s role continues as she nourishes the infant with milk produced in her breasts. The breasts are usually considered accessory reproductive organs. The clitoris is composed of erectile tissue and is located at the anterior portion of the female external genitalia. Although not essential for reproduction, the clitoris is important in providing a woman’s pleasure during the sexual act. The external genitalia consist of fatty tissue called the mons pubis and outer and inner folds of tissue, called the labia majora and labia minora, respectively. The opening of the urethra is located between the vagina and the clitoris. Internal female reproductive anatomy is shown in Figure 20-2.



