Chapter 14 The gastrointestinal and biliary system
Diarrhoea
The first line treatment is oral rehydration therapy using sugar-salt solutions, often with added starch, and the use of gruel rich in polysaccharides (e.g. rice or barley ‘water’) is an effective measure. The polysaccharides of rice (Oryza sativa) grains are hydrolysed in the GI tract; the resulting sugars are absorbed because the co-transport of sugar and Na+ from the GI lumen into the cells and mucosa is unaffected. Rice suspensions thus actively shift the balance of Na+ towards the mucosal side, enhance the absorption of water and provide the body with energy, and the efficacy of rice starch has been demonstrated in several clinical studies. The treatment of diarrhoea in adults, particularly for travellers, may also include opiates or their derivatives, to reduce gastrointestinal motility. Many classical anti-diarrhoeal preparations contain opium extracts, or the isolated alkaloids morphine and codeine (e.g. kaolin and morphine mixture, codeine phosphate tablets), although these are controlled by law in some countries. Opioid derivatives such as loperamide, which have limited systemic absorption and, therefore, fewer central nervous system side effects, have superseded these agents to some extent but the natural substances are still used and are highly effective. Dietary fibre, including that found in bulk-forming laxatives (qv) can also be used to treat diarrhoea; in this case, the fibre is taken with only a small amount of water. There are other plant drugs which act in varying ways (for review see Palumbo 2006).

Tannin-containing drugs
Tannins are astringent, polymeric polyphenols, and are found widely in plant drugs. The most important herbs used in the treatment of diarrhoea include Greater Burnet, Sangisorba officinalis L., Black Catechu, Acacia catechu Willd., Oak bark, Quercus robur L., Tormentil, Potentilla erecta (L.) Rausch., and even tea and coffee; however, many others are used in different countries (Palumbo 2006). Tannin-containing drugs are generally safe, but care should be taken with concurrent administration of other drugs since tannins are not compatible with alkalis or alkaloids, and form complexes with proteins and amino acids.
Constipation
Bulk-forming laxatives
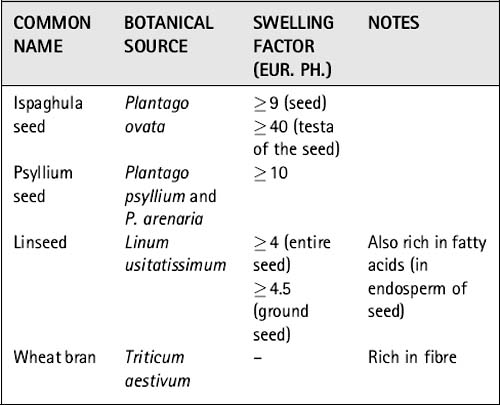
Bulking agents can be distinguished from swelling agents in that bulking material contains large amounts of fibre, whereas swelling material is generally composed of plant material (seeds) with a dense cover of polysaccharides on the outside. Both types of medicinal drugs may swell to a certain degree by the uptake of water, but swelling agents in the strict sense include only medicinal plants that form mucilage or gel. The swelling factor (which compares the volume of drug prior to and after soaking it in water) is an indicator of the amount of polysaccharides present in the drug and is generally used as a marker for the quality of bulk-forming laxatives. The European Pharmacopoeia requires a minimal value of the swelling factor for each agent, and the swelling factors of the phytomedicines detailed below are shown in Table 14.1. Preparations of bulk-forming laxatives are always taken with plenty of water. They can, paradoxically, be used to treat diarrhoea if given with very little fluid; they then absorb the fluid from the lumen and increase the consistency of the stool.



Stimulant laxatives
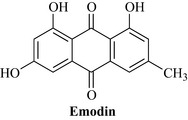
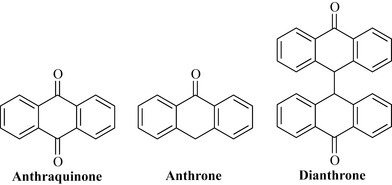
Stimulant laxatives are derived from a variety of unrelated plant species, which only have in common the fact that they contain similar chemical constituents. These are anthraquinones such as emodin (Fig. 14.1) and aloe-emodin, and related anthrones and anthranols. Anthraquinones are commonly found as glycosides in the living plant. Several groups are distinguished, based on the degree of oxidation of the nucleus and whether one or two units make up the core of the molecule. The anthrones are less oxygenated than the anthraquinones and the dianthrones are formed from two anthrone units (Fig. 14.2). Studies using dianthrone glycosides such as sennosides A and B suggest that most of these compounds pass through the upper GI tract without any change; however, they are subsequently metabolized to rhein anthrone in the colon and caecum by the natural flora (mainly bacteria) of the GI tract. Anthranoid drugs act directly on the intestinal mucosa, influencing several pharmacological targets, and the laxative effect is due to increased peristalsis of the colon, reducing transit time and, consequently, the re-absorption of water from the colon. Additionally, the stimulation of active chloride secretion results in an inversion of normal physiological conditions and a subsequent increased excretion of water. Overall, this results in an increase of the faecal volume with an increase in the GI pressure. These actions are based on the well-understood effects of chemically defined constituents; consequently, phytomedicines containing them are usually standardized to specified anthranoid content (see Chapter 9).
Frangula, Rhamnus frangula L. (Frangulae cortex); buckthorn, R. cathartica L. (Rhamni cathartici cortex) and cascara, R. purshiana DC. (Rhamni purshiani cortex) 
Constituents
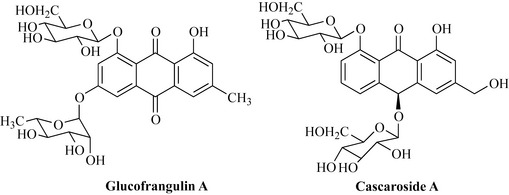
R. frangula. Glucofrangulin A (Fig. 14.3) and B, which are diglucosides differing only in the type of sugar at C6.
R. cathartica. Emodin, aloe-emodin, chrysophanol and rhein glycosides, frangula-emodin, rhamnicoside, alaterin and physcion.
R. purshiana. Cascarosides A (Fig. 14.3), B, C, D, E and F (which are stereoisomers of aloin and derivatives), with minor glycosides including barbaloin, frangulin, chrysaloin, palmidin A, B and C and the free aglycones.
Senna, Cassia senna L. and C. angustifolia Vahl (Senna) (Sennae fructus, Sennae folium)
Constituents
Leaf. Sennosides A and B (Fig. 14.4), which are based on the aglycones sennidin A and sennidin B; sennosides C and D, which are glycosides of heterodianthrones of aloe-emodin and rhein; palmidin A, rhein anthrone and aloe-emodin glycosides and some free anthraquinones. C. senna usually contains greater amounts of the sennosides.
Fruit. Sennosides A and B and a related glycoside sennoside A1. The sennosides, which are dianthrones, differ in their stereochemistry at C10 and C10′, as well as in their substitution pattern. C. senna usually contains greater amounts of the sennosides.
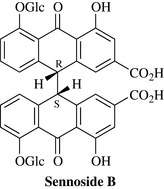
The structure of sennoside B is given in fig. 14.4. The Eur. Ph. standard is for a glycoside content of not less than 2.5% for the leaf, 3.5% for C. senna fruit and 2.2% for C. angustifolia fruit, calculated as sennoside B. Other secondary metabolites such as flavonoids, tannins and bitter compounds are also present but not defined in the standard. The way in which the plant material is dried has a strong influence on the amount of glycosides and accordingly on the quality of the product (see above).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


