Regulation of digestion
Storage and use of nutrients
Electrolyte and water metabolism
Growth and development
Reproduction
Synthesis, storage, and secretion of hormones.
TABLE 9-1 Endocrine Glands, Hormones, and Target Cells | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
the system is called a portal venous system. Thus, the hypothalamus and the anterior pituitary are connected by the hypothalamic-anterior pituitary portal blood flow system. Because this blood has already been used by the hypothalamus, it is poorly oxygenated but rich in hormonal messages put out by the hypothalamus into the median eminence (see later). The anterior pituitary is, therefore, a major target organ for hypothalamic hormones and responds to these hormones with the release of its own hormones that stimulate various glands or produces a primary effect on cells with mediation of other endocrine glands.
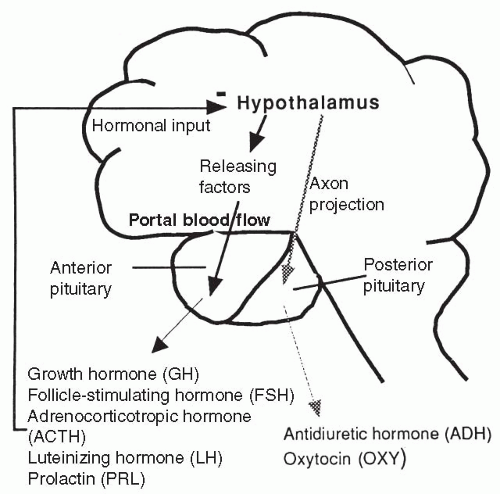 FIGURE 9-1 The hypothalamic-pituitary system. The hypothalamus is connected through the blood to the anterior pituitary while the posterior pituitary is a neural outgrowth. |
called vasopressin, and oxytocin. The hypothalamus sends these hormones in axon projections through the infundibular stem to the infundibular process. They are stored there until the hypothalamus stimulates them to be released into the general circulation. Thus, the hormones released by the posterior pituitary are hypothalamic in origin and depend on the hypothalamus for their release.
the amino acid tyrosine. A fourth category, the fatty acid derivatives, includes the retinoids and eicosanoids.
membrane permeability. TH travels in the blood mostly bound to carrier proteins with a smaller amount circulating free. Once at the target cell, free TH crosses the cell membrane and binds to the nuclear DNA, directly affecting DNA transcription. Therefore, free hormone, although lesser in quantity, is the active hormone. Amine hormones include aldosterone, glucocorticoids, androgens, and estrogens.
tissue to hormonal stimulation increases the further release of that hormone. The feedback mechanism is a series of reactions that work to achieve homeostasis by neuroregulatory mechanisms. The central nervous system (CNS) receives input that is transmitted to the hypothalamus. The hypothalamus then produces and releases either releasing or inhibiting factors that are transported to the pituitary. In the pituitary, releasing or inhibiting factors release or inhibit specific hormones. The anterior pituitary responds by controlling secretion of hormones from target organs or tissues.
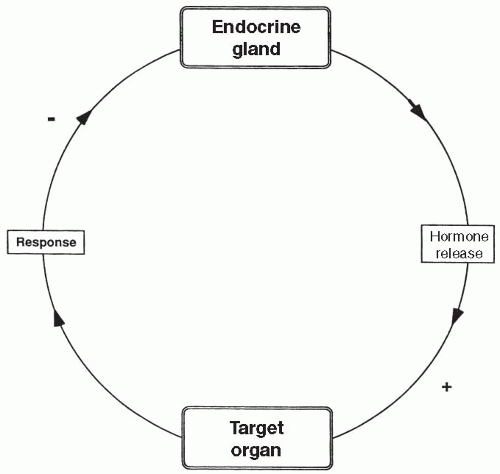 FIGURE 9-2 A typical negative feedback cycle in which an endocrine gland releases a hormone, which then stimulates (+) its target organ to respond in such a way that further secretion of the hormone by the endocrine gland is reduced (−). |
called thyroglobulin, which is synthesized in the thyroid gland and contains the amino acid tyrosine. These iodine-containing complexes are called iodotyrosines. Two iodotyrosines then combine to form two types of circulating TH, called T3 (triiodothyronine) and T4 (thyroxine). T3 and T4 differ in the total number of iodine molecules they contain (three for T3 and four for T4). Approximately 90% of the TH released into the bloodstream is T4, but T3 is physiologically more potent. A diet adequate in iodine and protein is necessary for T3 and T4 to be produced in adequate amounts. TH is stored in the thyroid gland as a colloid compound until needed. In passage through the liver and kidney, most T4 is converted to T3. T3 and T4 are carried to their target cells in the blood bound to a plasma protein, but enter the cell as free hormone. T3 and T4 collectively are referred to as TH.
Stimulates metabolic rate of all target cells by increasing the metabolism of protein, fat, and carbohydrate (primary function).
Stimulates the rate of the sodium-potassium pump in its target cells.
Increases utilization of energy by the cells, thereby increasing basal metabolic rate (BMR), burning calories, and increasing heat production by each cell (as a result of the two effects listed above).
Increases sensitivity of target cells to catecholamines, thus increasing heart rate and causing heightened emotional responsiveness.
Increases rate of depolarization of skeletal muscle, which increases the speed of skeletal muscle contractions, often leading to a fine tremor.
Essential for normal growth and development of all cells of the body and is required for the function of GH.
Increases red blood cell production.
levels of TH. When the secretion of TRH is stimulated by cold temperature, the result is an increase in TH, which increases BMR, thereby increasing body heat and reducing the demand for a further increase in TRH (Fig. 9-3). This is an example of negative feedback.
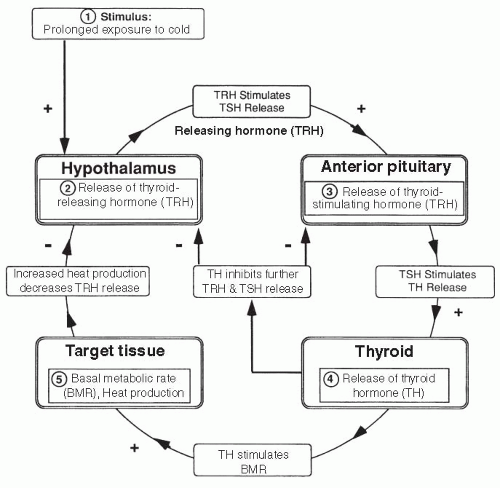 FIGURE 9-3 Feedback: thyroid hormone. |
Increase the level of blood glucose by stimulating gluconeogenesis (conversion in the liver of fats and proteins into glucose).
Increase blood glucose levels by stimulating muscle, adipose (fat), and lymphatic tissues to use free fatty acids for energy instead of glucose.
Stimulate protein breakdown and inhibit protein synthesis in all body cells.
Stimulate hunger, promote fat buildup in the trunk and face, and inhibit growth by suppressing GH and antagonizing the effects of GH on protein synthesis.
Increase the effect of GH on adipose tissue and increase the effect of TH on its target tissues.
Increase the effects of the catecholamines, causing increased heart rate and blood pressure.
Nonmetabolic effect that occurs with high circulating levels of cortisol include inhibition of immune and inflammatory functions by blocking almost every component of the immune and inflammatory responses including depressed cytotoxic T-cell function and suppression of the production, release, and activation of many chemical mediators of inflammation, including interleukins, prostaglandins, and histamine. Levels of cortisol high enough to inhibit immune and inflammatory function may be reached with pharmacologic administration of cortisol for immunosuppression, with tumors of the adrenal gland, or with long-term stress.
Major effect on emotional stability and mood.
children. High levels of ACTH can result in masculinization of women and children. ACTH is similar in structure to another anterior pituitary hormone, melanin-stimulating hormone (MSH), which causes the cells of the skin to produce the tanning substance melanin. High levels of ACTH can have crossover effects on the skin and cause bronzing. A limited amount of ACTH appears essential for the synthesis of another adrenal cortical hormone, aldosterone. Without aldosterone, salt wasting and death occur.
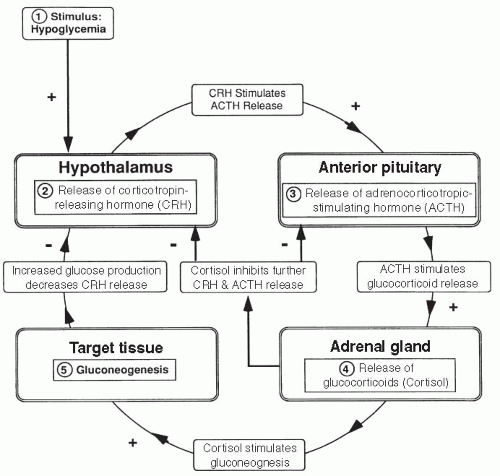 FIGURE 9-4 Feedback: glucocorticoids. |
Increases protein synthesis in all cells of the body, especially muscle cells.
Stimulates the growth of cartilage and activity of osteoblasts, the boneproducing cells of the body.
Essential for longitudinal bone growth and for the continual remodeling of bone which occurs throughout life. Effects of GH on bone and cartilage occur through intermediary peptides, called somatomedins or insulin-like growth factors (IGFs), released from the liver in response to GH.
Directly stimulates the growth of almost all other organs of the body, including the heart muscle, skin, and endocrine glands.
Causes breakdown of fats and subsequent use of fatty acids for energy. Because fats are being used as an energy source, GH results in increased circulating blood glucose.
Induces insensitivity to insulin. With decreased sensitivity to insulin, most cells will not transport glucose intracellularly, further increasing plasma glucose levels.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


