Chapter 6 The cardiovascular system
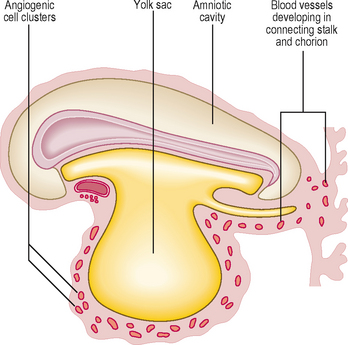
One of the first systems to develop in the embryo is the cardiovascular system because of the need to transport oxygen to embryonic cells. In the early embryo, nutrients are derived from trophoblastic digestion of the uterine mucosa, then via diffusion from the contents of the yolk sac. This soon becomes inadequate for the needs of the rapidly growing embryo. As the number of cells in the embryo increase most of the cells lose contact with a surface for diffusion to occur. The initial components of the cardiovascular system appear as angiogenic cell clusters in the extra-embryonic mesoderm lining the yolk sac (Fig. 6.1). These give rise to channels that extend into the embryo. The early embryonic blood vessels that appear around the neural plate in a horseshoe-shaped arrangement arise from the unsegmented mesoderm, which forms rostral to the prochordal plate. These clusters merge to form the cardiogenic area of the embryo, and the cells form tube-like structures, which initially become the paired heart tubes. The paired heart tubes bulge into the midline portion of the intra-embryonic coelom, which is the future pericardial cavity. The dorsal aortae develop on either side of the midline and connect with the heart tubes.
Heart tube formation
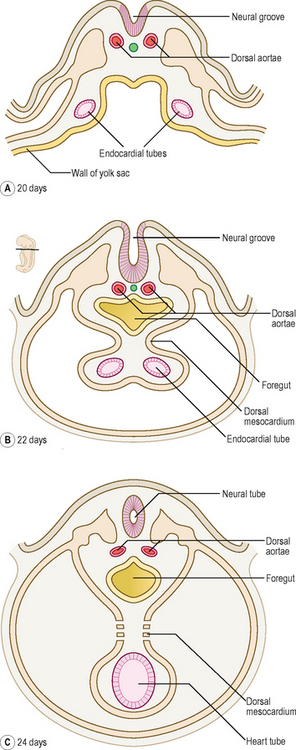
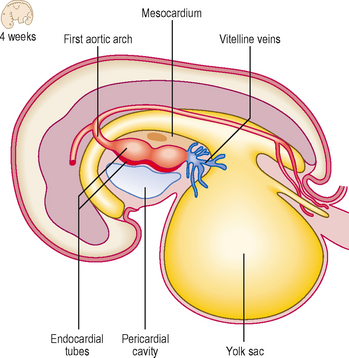
With the longitudinal and lateral folding of the embryo the heart tubes fuse to form a single tube, which is carried around to the region of the future thorax (Figs 6.1 and 6.2). The heart tube itself comprises an inner endothelial lining and an outer myocardial layer. The outer surface of the heart tube becomes invested in mesodermal tissue, which becomes the future visceral pericardium, or epicardium. This tube is retained within the pericardial cavity by a dorsal mesocardium which suspends the tube in much the same way as the gut tube is suspended in the peritoneal cavity. The heart tube is attached at its proximal and distal ends by the future ‘great’ arterial and venous vessels leaving and entering the heart respectively (Fig. 6.3). Soon, however, the dorsal mesocardium breaks down, leaving the heart tube attached merely at the margins of the pericardium. The heart tube itself differentiates during this time, to produce a thicker myocardium.
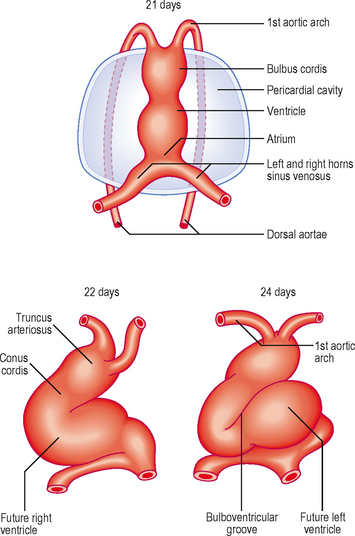
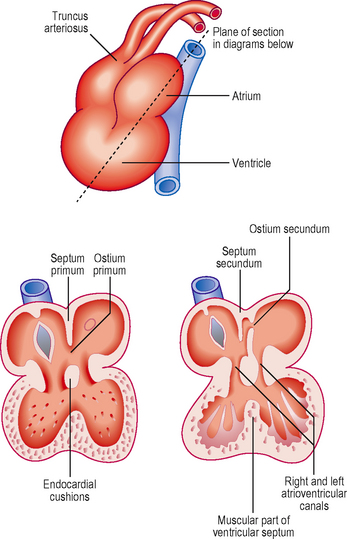
The heart tube continues to elongate in the pericardial cavity and develops a series of expansions. By day 23 it is too long to be accommodated in the volume available as a straight tube, thus it bends. This forms the cardiac loop (Fig. 6.4). The heart tube comprises an atrial portion, which initially is a single chamber, and a ventricular portion: the connection between the two becomes the narrow atrioventricular canal. In this region the atrioventricular valves will form later from structures called endocardial cushions. These are swellings of mesenchymal tissue, covered by endocardium. The canal connects the common atrium and primitive ventricle. Between the primitive ventricle and the arterial outflow is the bulbus cordis, which becomes the right ventricle. The left ventricle arises from the original primitive ventricle. The bends in the heart tube then occur at set places: the bulboventricular groove and the atrioventricular groove. The bulbus cordis becomes the conus cordis that leads from both future ventricles and is the outflow tract which leads on to the truncus arteriosus (Fig. 6.4). The truncus arteriosus continues to form the proximal parts of the aorta and pulmonary trunk. The proximal third of the bulbus cordis and the future right ventricle become trabeculated, whereas the conus remains smooth-walled, being associated with the outflow tracts.
Septation of the heart tube
In the atria, septation begins at about the fourth week. Initially, in the common atrium, a ridge develops in its roof. This is the septum primum (or primary septum) and it grows towards the endocardial cushions of the atrioventricular canal (Fig. 6.5). The opening that persists between the septum and the cushion is known as the ostium primum (or primary foramen). With further growth the ostium primum is closed, as it reaches the endocardial cushions. Before this closure occurs, however, small holes appear in the septum, which merge to form the ostium secundum (secondary foramen) (Fig. 6.5). By this means blood is able to flow between the two atria, an important feature of the fetal circulation (see later). Whilst the septum primum develops, another septum begins to form immediately to the right of the septum primum, the septum secundum (secondary septum). This grows over the septum primum, but never completely divides the atria, and leaves the opening of the foramen ovale (Fig. 6.5). The septum primum filling the foramen becomes the valve of the foramen ovale. This constitutes a vital mechanism for enabling circulation of blood from the right side of the heart, which contains oxygenated blood from the placenta, to pass into the systemic circulation, without passing through the pulmonary circulation. The pressure of blood on the right side of the heart is thus sufficiently high to force open the flap valve and allow the blood into the left atrium. After birth, air breathing commences and the pulmonary circulation begins, causing pressure to rise on the left side of the heart. The effect of this is to close the flap valve. In most people this results in the formation of a complete septum, the interatrial septum. In up to 20% of individuals, however, this is an incomplete seal, and may be opened with a probe, hence probe patency of the foramen ovale. Despite this, it is still a functional septum, allowing no passage of blood from the right to the left side. After birth, with the closure of the foramen ovale, the resulting central depression in the interatrial septum is known as the fossa ovalis.
 Clinical box
Clinical boxThe heart tube can loop to the left rather than the right, resulting in the anomaly of dextrocardia in which the heart comes to lie on the right hand side of the thorax, not the left. The condition may accompany situs inversus, a condition in which there is a complete mirror-image reversal of the internal organs of the thorax and abdomen. Such a condition is compatible with normal functioning, though there is an increased risk of volvulus (see Chapter 7) in the gastrointestinal tract.
Septum formation in the ventricle
The ventricles increase in size and internal volume due to growth of the myocardium. The ventricular wall becomes remodelled, leading to trabeculation. Tissue develops from the floor of the ventricles, midway between the right and left sides, and grows towards the endocardial cushions. This is the muscular component of the interventricular septum (Fig. 6.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


