Problem 5 Swelling in the neck in a 58-year-old man
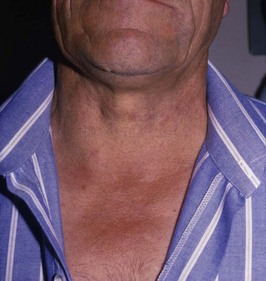
A 58-year-old man presents with a 6 month history of a swelling in the neck. This has been getting slowly bigger and is not painful. He has no other symptoms and the history is otherwise unremarkable. The swelling is shown in Figure 5.1. While taking the history you do, however, notice the swelling moves upwards on swallowing.
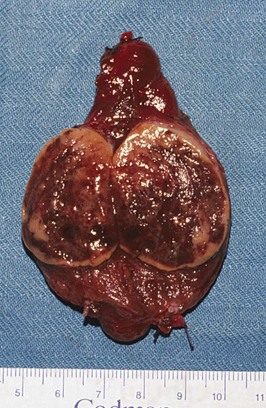
The patient undergoes a right thyroid lobectomy and makes an uneventful recovery.
Answers
A.2 You will want to know about the following:
• Is there a goitre which has either increased or decreased in size, or perhaps increased in size rapidly, suggesting bleeding or malignancy?
• Are there any symptoms suggestive of local pressure effects on adjacent structures in the neck (local pressure is common and often manifests as the inability to lie flat in bed at night, dysphonia, dysphagia, dyspnoea, noisy breathing)?
• Are there any symptoms suggestive of excessive thyroid hormone production (thyrotoxicosis)? This may occur in cases of toxic adenoma or from a dominant nodule within a multinodular goitre which is toxic. Alternatively the thyroid mass may be incidental to underlying Graves’ disease, but the presence of thyrotoxicity may modify the treatment plan.
• Specific enquiry of overactivity will include symptoms related to the metabolic, cardiovascular, neuropsychiatric and ocular manifestations of thyrotoxicosis. These would include increased appetite, weight loss, palpitations, altered bowel habit, temperature sensitivity, tremor, nervousness, muscle weakness, tiredness, low efficiency, anxiety, irritability and excessive sweating.
• An ophthalmic history should make note of any deterioration in vision or any sense of grittiness and diplopia.
• Thyroid nodules may be associated with hypothyroidism in the setting of Hashimoto’s thyroiditis. Specific features of hypothyroidism, such as intolerance of cold, constipation, tiredness, poor appetite, weight gain, forgetfulness, dryness of the skin and hair, a general slowing down mentally and physically, menorrhagia, symptoms of carpal tunnel syndrome, and symptoms of anaemia may be present.
• Is there a family history of thyroid cancer (particularly medullary and papillary thyroid cancer)?
• Has there been any previous exposure to ionizing radiation (especially in childhood) to the neck to treat conditions such as acne, tonsillitis, thymic enlargement or excessive facial hair?
• Has the patient lived in an area of endemic goitre or does he have a family history of multinodular goitre.
• Pain in the goitre is uncommon but may suggest haemorrhage into a nodule or subacute thyroiditis or rarely malignancy.
• The patient is examined with adequate exposure, free of clothing in the region of the neck, and in the sitting position.
• Is the goitre diffuse, i.e. does it affect the whole gland, or is there an apparently solitary nodule within an otherwise normal thyroid gland?
• The specific features of the thyroid mass are noted and should include site, shape, surface, consistency and tenderness.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


