The human liver is the largest internal organ in the body. It is estimated to weigh 0.2% to 0.3% of ideal body weight, or approximately 1400 to 2100 g in an otherwise healthy adult patient,1 depending on age, sex, and various disease processes.
The liver sits in the right upper quadrant of the abdomen, beneath the diaphragm, and is sheltered by the ribs.
In broad terms, the liver extends from the right 5th intercostal space superiorly to the edge of the costal margin inferiorly. A liver palpable below the costal margin often is a sign of hepatomegaly.
The left lobe of the liver extends beyond the midline and can reach as far left as midclavicular line.
Its location relative to external landmarks is neither consistent nor static and can vary depending on patient position, individual anatomy, and respiratory cycle. This must be taken into account when performing percutaneous procedures; radiographic guidance is essential.
Liver dimensions vary depending on age, gender, and disease states. Average dimensions are presented in Table 1.
The right and left hemilivers are anatomically and spatially divided by Cantlie’s line, which runs from the fundus of the gallbladder to the suprahepatic inferior vena cava (IVC). Within the substance of the liver, the middle hepatic vein courses along this same path and is the true division of the right and left hemilivers (FIG 1).
In 1954, Couinaud2 published his seminal work, Le Foie: Études Anatomiques Et Chirurgicales, in which he classified the liver into segments, each with their own inflow, outflow, and biliary drainage (FIG 2). He based his segments on the arborization of the portal vein within the liver. These segments begin with the caudate lobe (segment 1) and continue in a clockwise fashion from left to right.
Table 1: Average Dimensions of the Adult Liver | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
Goldsmith and Woodburne4 divided the liver into the caudate lobe and four distinct segments:
Left lateral (Couinaud segments 2 and 3)
Left medial (Couinaud segment 4)
Right anterior (Couinaud segments 5 and 8)
Right posterior (Couinaud segments 6 and 7)
Bismuth divided the liver based on fissures: three vertical lines corresponding to the divisions made by the three major hepatic veins.5
The fourth fissure, named the transverse fissure, is based on the level of the portal vein bifurcation within the liver and divides the “upper” liver from the “lower” liver.
Bismuth identified eight subsegments:
Caudate lobe (Couinaud segment 1)
Left superior subsegment (Couinaud segment 2)
Left inferior subsegment (Couinaud segment 3)
Left medial subsegment (Couinaud segment 4)
Right anterior inferior subsegment (Couinaud segment 5)
Right posterior subsegment (Couinaud segment 6)
Right posterior superior subsegment (Couinaud segment 7)
Right anterior superior subsegment (Couinaud segment 8)
Due to the confusion between various classifications, the International Hepato-Pancreato-Biliary Association (IHPBA) formed a committee in 1998 to delineate an accepted and
universal terminology to describe hepatic anatomy and, more specifically, hepatic resections.6 In 2000, their terminology was published. In it, a nomenclature for anatomic terminology and that of surgical resection were clearly delineated (Table 2).
 FIG 1 Axial CT image showing the MHV, which separates the right and left hemilivers. The IVC, left hepatic vein (LHV), and the branching of the right hepatic vein (RHV) are also shown. |
The caudate lobe is distinct in many ways. Because of its distinct inflow, outflow, and drainage, it is sometimes termed “the third lobe of the liver.”
Embryologically, it is derived from the right lobe,7 laying on the posterior surface of the right hemiliver, bordered on the left by the ligamentum venosus. It is bordered superiorly by the hepatic veins as they enter the IVC and posteriorly by the IVC itself. Inferiorly, it is bordered by the hilum of the liver and the bifurcation of the left and right portal veins.
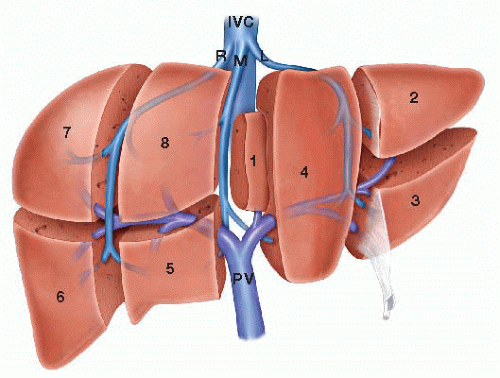
FIG 2 Diagram showing the segments (numbered 1 to 8) of the liver as described by Couinaud. The IVC as well as the right (R), middle (M), and left (L) hepatic veins. The portal vein (PV) is also shown. (From Smadja C, Blumgart L. The biliary tract and the anatomy of biliary exposure. In: Blumgart L, ed. Surgery of the Liver and Biliary Tract. New York, NY: Churchill Livingstone; 1994:11-24.)
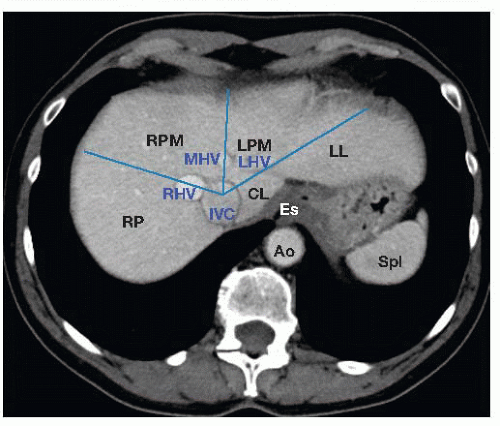
FIG 3 Axial CT image, venous phase, showing the right (RHV), middle (MHV), and left (LHV) as they enter the inferior vena cava (IVC). Blue lines show approximate direction of hepatic veins as they traverse the liver. Individual liver sectors are labeled (RL, right lateral; RPM, right paramedian; LPM, left paramedian; LL, left lateral). Also labeled are the caudate lobe (CL), esophagus (Es), aorta (Ao), and spleen (Spl).
Anatomically, there are three portions to the caudate lobe (FIG 4), each based on the portal inflow:8
The Spiegelian lobe (or Spiegel’s lobe)
The paracaval portion (or Couinaud’s segment 9)
The caudate process
Table 2: The Brisbane 2000 Terminology of Liver Anatomy and Resections
Anatomical Term*
Couinaud Segments
Surgical Resection Term
Based Upon
Right Liver Right Hemiliver
5-8
Right Hepatectomy Right Hemihepatectomy
Midplane of liver
Left Liver Left Hemiliver
2-4
Left Hepatectomy Left Hemihepatectomy
Right Anterior Section
5, 8
Right Anterior Sectionectomy
Hepatic artery and biliary duct divisions
Right Posterior Section
6, 7
Right Posterior Sectionectomy
Left Medial Section
4
Left Medial Sectionectomy
Left Lateral Section
2, 3
Left Lateral Sectionectomy
Right Anterior Sector Right Paramedian Sector
5, 8
Right Anterior Sectorectomy Right Paramedian Sectorectomy
Portal vein divisions
Right Posterior Sector Right Lateral Sector
6, 7
Right Posterior Sectorectomy Right Lateral Sectorectomy
Left Medial Sector Left Paramedian Sector
3, 4
Left Medial Sectorectomy Left Paramedian Sectorectomy
Left Lateral Sector Left Posterior Sector
2
Left Lateral Sectorectomy Left Posterior Sectorectomy
* Terms that include segment 1 should be stated as such (i.e., left hepatectomy extended to segment 1).
Adapted from Strasberg SM. Terminology of liver anatomy and resections: the Brisbane 2000 terminology. In: Clavien PA, Sarr MG, Fong Y, eds. Atlas of Upper Gastrointestinal and Hepato-Pancreato-Biliary Surgery. Berlin: Springer; 2007:313-317.

FIG 4 A. Axial CT image showing the caudate lobe. The caudate process (CP) is bounded by the anterolateral surface of the IVC, the left portion of liver hilum, and the left hepatic vein (not shown). Segment 9 (Sg 9) is known as the paracaval process and is bounded by the anterior surface of the IVC, the middle hepatic vein (MHV), and the right hepatic vein (RHV). Also shown is the portal vein (PV). B. Axial CT image (slightly more caudal than in [A]) showing Spiegel’s lobe (Sp)—also known as segment 1—as it wraps around the medial aspect of the IVC.
Surgically, the caudate can be divided in two: segment 1 (Spiegel’s lobe) and so-called segment 9 (paracaval portion and caudate process) (FIG 5).
The use of terminology related to Couinaud segment 9 is often dropped from the literature and this term is neither universally accepted nor used.
The paracaval portion, which projects medially, can circumferentially wrap around the IVC.9 This can be misinterpreted on computed tomography (CT) scan as an enlarged lymph node, and the surgeon should be aware of this to avoid inappropriate preoperative staging of a patient.
The caudate derives its portal inflow from the left and right portal veins; venous drainage is directly into the IVC via multiple small caudate veins. Thus, in diseases of hepatic venous obstruction, such as Budd-Chiari syndrome, it will hypertrophy and provide alternate routes for obstructed hepatic venous flow.
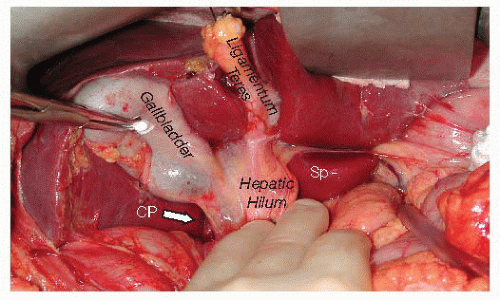 FIG 5 In situ photograph showing Spiegel’s lobe (Sp) and the caudate process (CP) in relation to the hepatic hilum. Also shown are the gallbladder and the ligamentum teres. |
The liver is covered by a thin membrane called Glisson’s capsule. This epithelial layer is contiguous with internal anatomy of the liver as sheaths around the portal veins, hepatic arteries, and bile ducts.10
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


