Spitz (Spindle and Epithelioid Cell) Nevi
Jessica M. Comstock, MD
David Cassarino, MD, PhD
Key Facts
Clinical Issues
Benign melanocytic tumor
Most common in children and young adults
Common sites: Extremities, especially thigh
Pink or flesh-colored, dome-shaped dermal papule or nodule
Microscopic Pathology
Junctional, compound, and dermal forms
Symmetric, well circumscribed
Varying proportions of spindled and epithelioid melanocytes
Spindle cells much more common
Epithelioid cells usually dispersed individually throughout lesion
Melanocytes “mature” by becoming smaller from superficial to deep
Kamino bodies: Eosinophilic globules at dermal-epidermal junction
Artifactual clefting of papillary dermal nests from overlying epidermis often present
Can show atypical features (atypical Spitz nevus/tumor)
Top Differential Diagnoses
Spitzoid melanoma; findings suspicious for melanoma include
Patient > 10 years old
Lesion > 1 cm
Ulceration and increased mitoses present
Asymmetry and poor circumscription
Subcutaneous involvement
Pigmented spindle cell nevus of Reed
Conventional melanocytic nevi
 A pink papule, typical of a Spitz nevus, is shown on the face of a child. (Courtesy R. J. Antaya, MD.) |
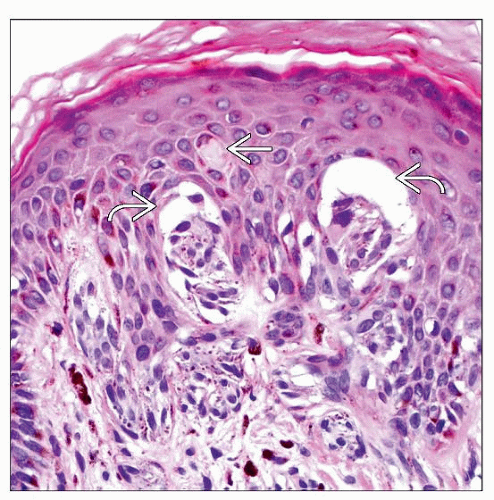 High-power examination of a Spitz nevus shows small nests of epithelioid to spindled melanocytes with overlying artifactual clefting  and an eosinophilic Kamino body and an eosinophilic Kamino body  . . |
TERMINOLOGY
Synonyms
Spindle and epithelioid cell nevus
Spindle cell nevus
Epithelioid cell nevus
Nevus of large spindle &/or epithelioid cells
Benign juvenile melanoma (outdated term)
CLINICAL ISSUES
Site
Extremities, especially thigh
Trunk
Head and neck
Presentation
Most common in children and young adults
0.5-1% of all nevi in children and adolescents
May occur at all ages
Solitary
Can be clustered or disseminated
Treatment
Complete conservative excision
Prognosis
Benign
Low recurrence rate, even after incomplete excision
MACROSCOPIC FEATURES
General Features
Dome-shaped dermal nodule
Pink or flesh-colored
Often misdiagnosed clinically as hemangioma or pyogenic granuloma
Size
Usually < 1 cm
MICROSCOPIC PATHOLOGY
Histologic Features
Junctional, compound, and dermal forms
Most common type is compound with prominent dermal component
Symmetric, well-circumscribed proliferation
Usually no lateral extension of junctional nests beyond dermal component
Varying proportions of spindled and epithelioid melanocytes
Spindle cells more common in most cases
Completely spindle cells in ~ 45% of Spitz nevi
Mixed spindle and epithelioid cells in ~ 35%
Only epithelioid cells in ~ 20%
Epithelioid cells usually dispersed individually throughout lesion
Spindle cells are arranged in fascicles perpendicular to epidermis
Small clusters of melanocytes can be seen in epidermis
Can see pagetoid spread of a few single melanocytes
Artifactual clefting of junctional nests from overlying epidermis
Kamino bodies
Eosinophilic globules at dermal-epidermal junction
Important diagnostic clue, but may need step sections to find
PAS and trichrome positive
Melanocytes “mature” by becoming smaller from superficial to deep
Melanocytes taper to narrow point in deep dermis, forming upside-down triangle
Deep melanocytes may resemble ordinary nevus cells
Important clue for differentiating from melanoma
Other unique features
Vascular and sometimes edematous stroma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


