Solitary Rectal Ulcer Syndrome/Mucosal Prolapse
Julianne K. Purdy, MD
Key Facts
Clinical Issues
Rare; usually in young to middle-aged adults
Ulcer, polyp, erythema on anterior rectal wall
Rectal bleeding or straining with defecation
Microscopic Pathology
Fibromuscular obliteration of lamina propria, muscularis mucosa hypertrophy, & disorganization
Mild mucosal architectural distortion, reactive atypia, surface hyperplasia
Top Differential Diagnoses
Inflammatory bowel disease
Extensive chronic lamina propria inflammation
Rectal mucinous adenocarcinoma
Epithelium floating in irregular pools of mucin, cytologic atypia, desmoplasia
Adenoma, Peutz-Jeghers polyp, hyperplastic polyp
No fibromuscular obliteration of lamina propria; dysplasia (adenoma)
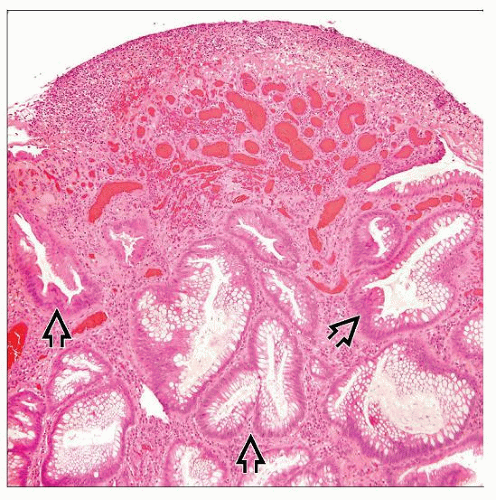 Hematoxylin & eosin shows polypoid ulcerated rectal mucosa with underlying fibromuscular proliferation in the lamina propria and serrated, branching, haphazardly arranged crypts  . . |
 Hematoxylin & eosin shows hypertrophied, disorganized smooth muscle of the muscularis mucosa  , extending up into the lamina propria between crypts , extending up into the lamina propria between crypts  . . |
TERMINOLOGY
Definitions
Solitary rectal ulcer syndrome (SRUS)
Chronic benign defecation disorder with histologic features of mucosal prolapse
ETIOLOGY/PATHOGENESIS
Contraction of Sphincter during Defecation
Excessive straining → compression of rectal wall, prolapse
Venous congestion, traction on submucosal vessels → poor blood flow → ischemia, ulceration
Direct Trauma
Digital evacuation of stool or reduction of rectal prolapse → direct trauma and ulceration
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


