Solitary Fibrous Tumor
Khin Thway, BSc, MBBS, FRCPath
Key Facts
Terminology
Fibroblastic mesenchymal tumor with prominent hemangiopericytic branching vascular pattern
Initially described in pleura
Occur in any location
Closely related tumors
Lipomatous hemangiopericytoma
Giant cell angiofibroma
Clinical Issues
Affects adults with equal sex distribution
Behavior difficult to predict from histological parameters
Long-term follow-up indicated
Microscopic Pathology
Fibroblasts with uniform small fusiform, ovoid, or sometimes spindled nuclei, in “patternless” distributions
Varying proportion of fibrous stroma
Prominent vascular pattern
Malignant SFT
Hypercellularity, atypia, mitoses > 4/10 HPF, necrosis, and infiltrative margins
Lipomatous hemangiopericytoma has admixed fat
Giant cell angiofibroma has spaces lined by multinucleated cells
Ancillary Tests
Characteristic diffuse immunoreactivity for CD34
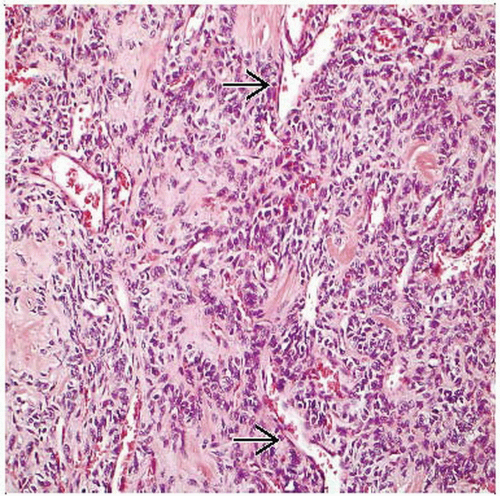 Hematoxylin & eosin shows a solitary fibrous tumor, with spindle to ovoid cells in a collagenous stroma and interspersed hemangiopericytic vessels  . . |
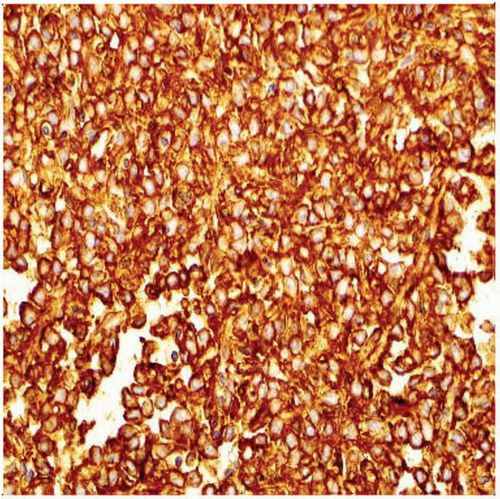 CD34 immunohistochemistry shows characteristic diffuse strong cytoplasmic and membranous positivity throughout the tumor. |
TERMINOLOGY
Abbreviations
Solitary fibrous tumor (SFT)
Synonyms
Localized fibrous mesothelioma, localized fibrous tumor, submesothelial fibroma, localized fibroma, subpleural fibroma
Definitions
Fibroblastic mesenchymal tumor with prominent branching (hemangiopericytoma-like) vascular pattern
Initially described in pleura but subsequently described in almost any organ or site
Many previously diagnosed soft tissue hemangiopericytomas are probably solitary fibrous tumors
Closely related tumors
Lipomatous hemangiopericytoma
Giant cell angiofibroma
ETIOLOGY/PATHOGENESIS
Unknown
Initially considered mesothelial
Now accepted as mesenchymal tumor
CLINICAL ISSUES
Epidemiology
Age
Adults (range: 20-70 years)
Occasionally in children and adolescents
Gender
M = F
Site
Deep soft tissue
Viscera
Subcutaneous tissue and very rarely at cutaneous sites
Head and neck, including orbit and intracranial sites
Extrapleural lesions more frequent than pleural
Presentation
Slow growing
Painless mass
Rarely paraneoplastic syndrome of hypoglycemia due to production of insulin-like growth factor
Treatment
Surgical approaches
Simple surgical resection for benign SFT
More extensive surgery for malignant SFT
Adjuvant therapy
Combination of radiation therapy and chemotherapy in malignant SFT
Prognosis
Long-term follow-up is mandatory due to unpredictable behavior of SFT
Most are benign
Up to 15% behave aggressively
Most tumors with histologically “benign” morphology do not recur or metastasize
Histologically malignant tumors usually behave aggressively
MACROSCOPIC FEATURES
General Features
Lobulated, circumscribed mass
Malignant tumors may be locally infiltrative
Firm gray-white or brown cut surface
Occasional cystic degeneration or hemorrhage
Size
1-20 cm (most 5-10 cm)
MICROSCOPIC PATHOLOGY
Histologic Features
Classically shows alternating cellularity, with variation between highly cellular and sparsely cellular areas
Fibroblasts with uniform small fusiform, ovoid, or sometimes spindled nuclei and scanty cytoplasm
Occasional multinucleate giant cells
Atypia is unusual
“Patternless” pattern of fascicles
Varying proportion of fibrous stroma
Frequent dense keloid-like hyalinization
Stroma may show cracking artifact
Amianthoid fibers rarely described
Myxoid or cystic change can occur
Prominent vascular pattern
Frequent perivascular hyalinization
Branching or staghorn-shaped large vessels
Mitotic figures and necrosis rare
Malignant solitary fibrous tumor
No precise correlation between morphology and behavior, but the following features suggest malignancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


