52 Solid tumours
Epidemiology
Prostate cancer is now the most common cancer in men (24%) followed by lung (15%) and bowel (14%) cancer. In women, breast cancer is the most common (31%) followed by bowel (12%) then lung (12%). However, there are regional variations. From 1979 to 2008, mortality rates from cancer fell by 20% (Cancer Research UK, 2010).
Aetiology
Environmental factors
Increasingly, lifestyle factors play a large part in the development of many cancers. Cigarette smoking has been identified as the single most important cause of preventable disease and premature death in the UK. The beneficial effect of stopping smoking on the cumulative risk of death from lung cancer reduces with increasing age (Doll et al., 2004). Smoking causes about 90% of lung cancer deaths, and the link between tobacco and cancer was established more than 50 years ago.
Table 52.1 lists a number of other factors which have been associated with cancer development.
Table 52.1 A–K of factors associated with specific cancer sites: An empirical basis for recommending lifestyle changes (Jankowski and Boulton, 2005)
| Factor | Associated cancer |
|---|---|
| Alcohol consumption >3 units a day | Most squamous cancers, especially bladder and oesophagus |
| Body mass index >25 and certainly >30 | All solid cancers |
| Cigarette smoking at any level (even passive smoking) | Bladder, lung, head and neck, oesophagus and oropharyngeal cancers |
| Diet, especially one that is high in fat | All solid cancers |
| Exercising <30 min a day | All solid cancers |
| Family history of cancer (in at least one first-degree relative and at least three people in two or more generations) | Inherited cancer syndromes, including breast, colorectal, diffuse gastric, ovarian, prostate and uterine cancers |
| Genital and sexual health (sexually transmitted infections) | Cervical cancer |
| Health-promoting drugs that may decrease global cancer risks (but need a careful risk/benefit analysis) | Colonic adenomas can be treated with low-dose aspirin but can have serious side effects Hormone replacement therapy linked with breast cancer |
| Intense sunburn | Melanoma |
| Job-related factors | Lung cancer (exposure to asbestos and particulates), skin cancer (contact with arsenic) |
| Known disease associations | Colorectal cancer has predisposing mucosal pathology – adenomas, coeliac disease, ulcerative colitis |
Genetic factors
A number of rare tumours are known to be associated with an inherited predisposition, where an individual is born with a marked susceptibility to cancer. This is due to the inheritance of a single genetic mutation which may be sufficient to greatly increase the risk of one or more types of cancer. Examples include the paediatric malignancies, Wilms’ tumour of the kidney and bilateral retinoblastoma, a rare cancer of the eye. Some common cancers such as breast, ovarian and colorectal cancer may also show a tendency to occur in families, but these represent a small proportion of the overall presentation of common cancers where identifiable risk factors are relevant in only 5–10% of cases, although when the genetic factor is present the cancers tend to have their onset at a younger age (Garber and Offit, 2005).
Screening and prevention
Chemoprevention
Another potential future development is the effect of aspirin as a chemopreventive agent for colorectal cancer. Maximal effect requires long-term use of high-dose aspirin that may increase the risk of gastro-intestinal bleeding. Non-steroidal anti-inflammatory drugs (NSAIDs) and selective cyclooxygenase-2 (COX-2) inhibitors may also be candidates for chemoprevention. However, the regular use of these drugs may also cause gastro-intestinal bleeding and increase the risk of cardiovascular events (Herszényi et al., 2008)
Cancer at the cellular level
Tumour suppressor genes
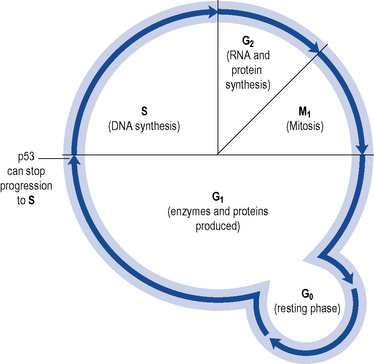
The p53 protein acts as a regulator of cell growth and proliferation and controls passage from G1 to S phase in cell division (see Fig. 52.1). Agents which damage DNA cause p53 to accumulate. This accumulation of p53 switches off replication in the cell, arresting the cell cycle and allowing time to repair. If repair fails, p53 may trigger cell suicide by apoptosis. Thus, p53 controls and halts the proliferation of abnormal cell growth.
Tumour growth
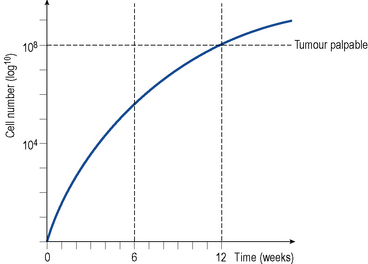
A solid tumour represents a population of dividing and non-dividing cells. The time it takes for a tumour mass to double is known as the doubling time. The latter will vary depending on the type of tumour but for most solid tumours it is about 2–3 months. In most solid tumours, the growth rate is very rapid initially (exponential growth) and then slows as the tumour increases in size and age, a pattern described as Gompertzian growth (see Fig. 52.2). The growth fraction is the percentage of actively dividing cells in the tumour, and this decreases with increasing tumour size.
Patient management
Clinical assessment
Tumour markers
Tumour markers are usually proteins associated with a malignancy and are clinically useful to:
They may be detected in a solid tumour, in circulating tumour cells in peripheral blood, in lymph nodes, in bone marrow or in other body fluids. A number of the tumour markers are presented in Table 52.2.
Table 52.2 Examples of tumour markers used in detection, diagnosis and monitoring
| Tumour marker | Indicative cancer |
|---|---|
| CA125 | Ovarian cancer, although non-specific |
| α-Fetoprotein (AFP) | Testicular tumour |
| β-Human chorionic gonadotrophin (β-HCG) | |
| 5-Hydroxyindole acetic acid (5HIAA) | Carcinoid tumours |
| Thyroglobulin | Thyroid cancer |
| α-Fetoprotein | Hepatocellular carcinoma |
| Prostate-specific antigen | Prostate cancer |
| Human chorionic gonadotropin | Gestational trophoblastic tumours |
Staging investigations
Since the cancer is often disseminated at the time of presentation, it is vital that patients undergo thorough staging investigations to establish the extent and nature of disease. This will determine the most appropriate treatment offered to the patient. Baseline investigations range from clinical examination, blood tests, liver function tests, diagnostic imaging such as chest and skeletal X-rays, ultrasound, computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET), depending on the disease type and likely pattern of spread. Clinical guidelines for staging and management of malignancies of the various body systems have been produced at local and national level in most developed countries, with relatively minor variations according to local custom and practice (e.g. NICE in UK, see http://www.nice.org.uk/ for guidance and NCI in USA, see http://www.cancer.gov/ for guidance).
Staging classification
Most tumours are classified according to the TNM (tumour–nodes–metastases) system where T (0–4) indicates the size of the primary tumour, N (0–3) the extent of lymph node involvement and M (0–1) the presence or absence of distant metastases. Each solid tumour site has a specific grading and staging classification such as Dukes staging in colorectal cancer (Cancer Research UK, 2009) and Gleason scoring for grading prostate cancer (Berney, 2007).
Performance status
The patient’s general level of fitness (performance status) at the time of diagnosis is often a surprisingly reliable indicator of prognosis independent of disease-related factors, and will help determine if they are likely to withstand intensive chemotherapy; this therefore influences the choice of treatment. A number of physical rating scales have been devised to assess performance status, including the Karnofsky performance index (Karnofsky and Burchenal, 1949) and the World Health Organization (WHO) performance scale (Box 52.1).
Box 52.1 Performance status scales
100 Normal, no complaints, no evidence of disease
90 Able to carry on normal activity, minor signs or symptoms of disease
80 Normal activity with effort, some signs or symptoms of disease
70 Cares for self, unable to carry on normal activity or do active work
60 Requires occasional assistance but is able to care for most of own needs
50 Requires considerable assistance and frequent medical care
40 Disabled, requires special care and assistance
30 Severely disabled, hospitalisation is indicated, although death is not imminent
20 Very sick, hospitalisation necessary, active supportive treatment is necessary
10 Moribund, fatal processes progressing rapidly
Prognostic factors
These are factors that can predict how the disease is likely to behave and determine an outcome in individual patients. For example, Table 52.3 lists prognostic factors in patients with colorectal cancer.
Table 52.3 Prognostic factors in patients with colorectal cancer
| Favourable | Unfavourable |
|---|---|
| Good performance status | Presence of nodal involvement |
| No penetration of the tumour through the bowel wall | Presence of distant metastases |
| Absence of nodal involvement | Bowel obstruction and bowel perforation |
| Absence of distant metastases |



