Problem 48 Severe dehydration in a young woman
An 18-year-old girl is brought into the emergency department by ambulance from a youth hostel. She is a backpacker and has been travelling around the country. She is drowsy and unable to give any history. Her airway is clear and her breathing is unhindered. She reacts purposefully to painful stimuli, moving all limbs, and grunts but does not speak. She opens her eyes briefly in response to you shouting her name.
There are a number of possible causes for this woman’s comatose state.
You have a working diagnosis for this patient who is critically ill.
The patient decides to curtail her backpacking holiday and return home.
Answers
A.1 Her Glasgow coma score is 11 (E4, V2, M5).
A.3 As part of the immediate management, the following must be undertaken:
• Insert an intravenous cannula and take blood for electrolytes, urea and creatinine, blood glucose, complete blood picture, lipase.
• Commence emergency resuscitation with intravenous infusion of isotonic saline. At least 1–1.5 litres should be given over the first hour.
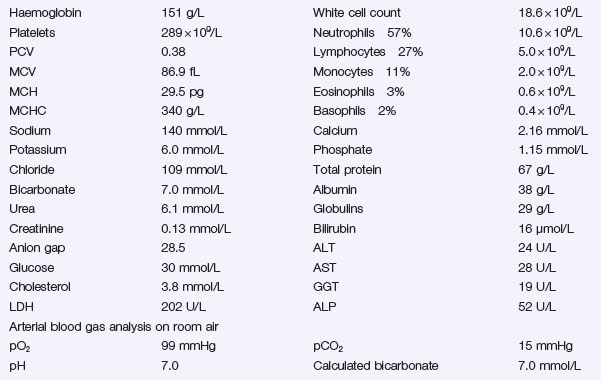
Metabolic acidosis can be divided into:
• High anion gap acidosis (addition of anions to the blood, e.g. ketoacidosis, lactic acidosis and salicylate or alcohol poisoning).
• Normal anion gap acidosis with a high chloride level, usually as a result of loss of alkali (bicarbonate), for example from the gut with severe diarrhoea or in renal tubular acidosis.



