Sessile Serrated Adenoma
Alexandros D. Polydorides, MD, PhD
Key Facts
Terminology
Serrated polyps: Saw-toothed epithelium (infolding)
HP, TSA, SSA/P, mixed adenoma-serrated polyps
Etiology/Pathogenesis
Inhibition of apoptosis/exfoliation of surface mucosa
“Serrated neoplasia pathway”
HP → SSA/P → TSA → serrated carcinoma
Silencing of DNA repair genes (MLH1, MGMT)
CpG island methylator phenotype (CIMP)
BRAF mutation (in up to 75%), MSI-high
Clinical Issues
2-10% of all colon polyps, 8-18% of serrated polyps
Usually right-sided (75%), large (> 1 cm), flat (sessile)
Large (> 1 cm) or right-sided SSA/P: Remove entirely
If not: Watchful, biopsy at short interval (1 year)
Microscopic Pathology
Dilatation, exaggerated serration down to crypt base
Branching, lateral growth along muscularis mucosae
Horizontal, L- or inverted T-shaped crypt bases
Mitoses asymmetrically extend to upper crypts
Inverted maturation: Goblet cells down to crypt base
Absence of thickened subepithelial collagen layer
Classic (overt) cytologic dysplasia generally not seen
Top Differential Diagnoses
Hyperplastic polyp
Serration usually confined to superficial crypts
Straight, tubular, narrow base (proliferation zone)
(Traditional) serrated adenoma
Exophytic configuration, surface epithelial tufting
Abundant eosinophilic cytoplasm, pencillate nuclei
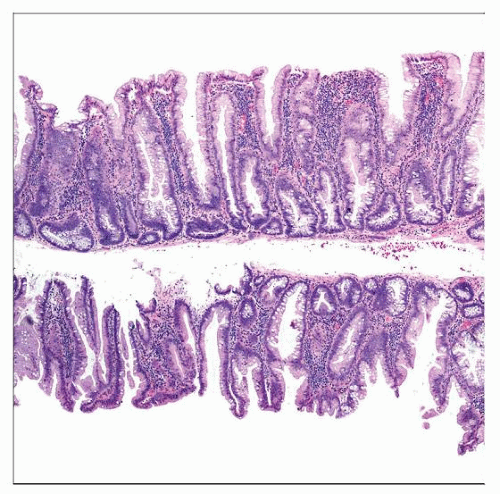 Hematoxylin & eosin shows a low-power view of 2 strips of a sessile serrated adenoma/polyp with flat (sessile) rather than pedunculated growth and absence of a stalk. |
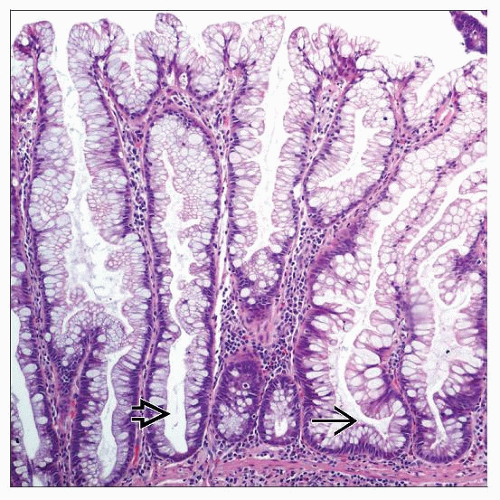 Hematoxylin & eosin shows a medium-power view of an SSA/P with characteristic architecture, including dilation  and branching and branching  of the epithelial crypts extending to the base. of the epithelial crypts extending to the base. |
TERMINOLOGY
Abbreviations
Sessile serrated adenoma/polyp (SSA/P)
(Traditional) serrated adenoma (TSA)
Hyperplastic polyp (HP)
Synonyms
Sessile serrated polyp, giant hyperplastic polyp, serrated polyp with abnormal proliferation
Definitions
SSA/P: Usually sessile, large, and right-sided polyps
Abnormal proliferation, architectural distortion
Dilation, branching extending to crypt base
Generally lack overt cytologic dysplasia
Serrated polyps: Saw-toothed epithelial infoldings
HP, TSA, SSA/P, and mixed adenoma-serrated polyps
ETIOLOGY/PATHOGENESIS
Recognized in Hyperplastic Polyposis
Emerging biologic characteristics, histologic features
Differs from classic HP; suggests distinct pathogenesis
Serrated (Sawtooth) Epithelium
Inhibition of apoptosis/exfoliation of surface mucosa
Expanded crypt proliferation, delayed cell maturation Abnormal Proliferation, “Dysmaturation”
Mitoses migrated upward, often in irregular manner
Higher on 1 side of crypt (asymmetric)
Distinct Molecular Abnormalities
High frequency of DNA methylation at CpG islands
BRAF-activating mutations (rather than KRAS)
Lack Conventional Cytologic Dysplasia
Thus, some prefer term “sessile serrated polyp”
May be low-grade TSA or HP-TSA intermediate
“Serrated Neoplasia Pathway”
Precursor of microsatellite instable (MSI) carcinoma
Nonsyndromic (non-HNPCC), MSI-high, right-sided
Progression: HP → SSA/P → TSA → carcinoma
Mixed adenoma-serrated polyps: Mostly TSA-SSA/P
Faster progression than classic adenoma → carcinoma
May explain “interval tumors” that occur between endoscopies
Lack APC/KRAS/p53 mutations or chromosomal instability
Has instead BRAF mutation (in up to 75%), MSI-high
Silencing of DNA repair genes (MLH1, MGMT)
CpG island methylator phenotype (CIMP)
MSI correlates with overt cytologic dysplasia in SSA/P
˜ 10-15% of colon cancers may arise in this setting
CLINICAL ISSUES
Epidemiology
Incidence
2-10% of all colon polyps, 8-18% of serrated polyps
Endoscopic Findings
Usually right-sided (75%), large (> 1 cm), flat (sessile)
Poorly circumscribed, smooth (mimic enlarged folds)
Natural History
Probable precursor to MSI-high carcinomas
Thus, some prefer term “sessile serrated adenoma”
Residual serrated polyps in ˜ 6% of colorectal cancers
In ascending colon, transition through adenoma
Underestimated (tumors outgrow precursor lesions)
Adenomatous change obscures original serration
Treatment
Options, risks, complications
Limited data, anecdotal experience
Large (> 1 cm) or right-sided SSA/P: Remove entirely
If not: Watchful, biopsy at short interval (1 year)
With cytologic dysplasia (adenomatous change)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


