Rosai-Dorfman Disease
Elizabeth A. Montgomery, MD
Key Facts
Terminology
Lesional histiocytes contain variable numbers of intact lymphocytes within their cytoplasm
Referred to as lymphophagocytosis or emperipolesis
Sinus histiocytosis with massive lymphadenopathy (term for disease involving lymph nodes)
Clinical Issues
Painless lymphadenopathy most frequent presenting symptom
Skin and soft tissue most common extranodal site
Poor prognosis correlates with widespread dissemination
Involves kidneys, lower respiratory tract, liver, and immunologic abnormalities or anemia
Most patients have complete & spontaneous remission
Some may experience recurrent or persistent but stable lymphadenopathy
Microscopic Pathology
Skin and soft tissue cases have more subtle histologic features than lymph node counterparts
Emperipolesis less conspicuous
Proliferating histiocytes frequently spindled
Majority of lesions label with S100
Vague storiform pattern
Scattered lymphoplasmacytic aggregates
Top Differential Diagnoses
Langerhans cell histiocytosis (LCH)
Juvenile xanthogranuloma
Disorders featuring granulomatous inflammation
Histiocytic sarcoma (histiocytic lymphoma)
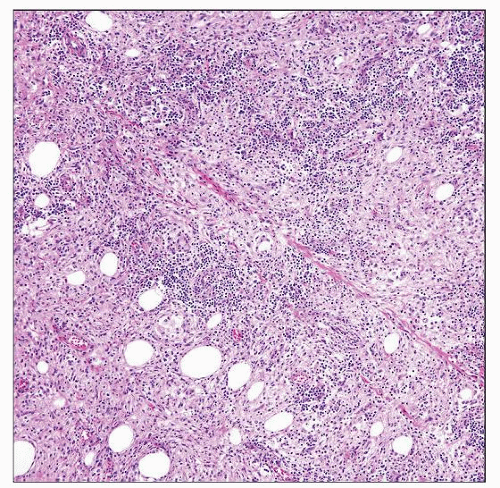 Histologic examination shows a low-power image of extranodal (soft tissue) Rosai-Dorfman disease. The proliferating histiocytes are spindled, infiltrating fat. Small lymphoid aggregates are present. |
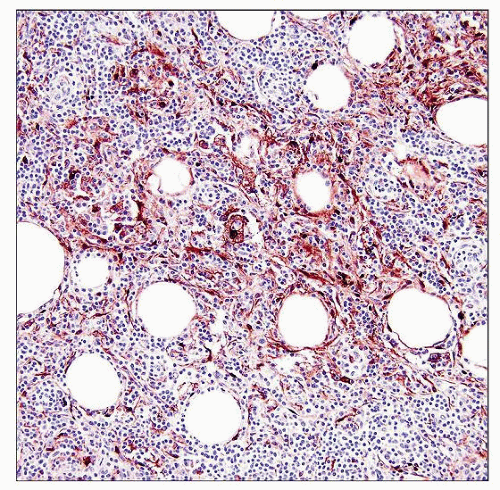 S100 protein shows labeling of the proliferating histiocytes. The staining pattern is not diffuse and must be correlated with the morphology. Some labeled cells are dendritic cells. |
TERMINOLOGY
Abbreviations
Rosai-Dorfman disease (RDD)
Synonyms
Sinus histiocytosis with massive lymphadenopathy (SHML)
Applies to disease involving lymph nodes
Definitions
Rare, acquired, nonmalignant proliferation of distinctive histiocytes that presents with lymphadenopathy or extranodal disease
Lesional histiocytes contain variable numbers of intact lymphocytes within cytoplasm
Phenomenon referred to as lymphophagocytosis or emperipolesis
Primarily in children and young adults
ETIOLOGY/PATHOGENESIS
Exuberant Hematopoietic Response to Undetermined Immunologic Trigger
Association with autoimmune lymphoproliferative syndrome has been described
Inherited disorder of lymphocyte-programmed cell death with mutations in death receptor genes that specifically eliminate apoptosis in lymphocyte subsets
Occurs primarily in early childhood
May represent acquired disorder of deregulation of apoptotic signaling pathways
Various infections associated with cases of RDD/SHML, but none proven as etiologic infectious agent
Parvovirus
Epstein-Barr virus
HHV6
Polyoma virus
CLINICAL ISSUES
Presentation
Varies with site
Painless lymphadenopathy is most frequent presenting symptom
Involves cervical region in up to 90% of patients
30-45% of patients have at least 1 site of extranodal involvement as well as lymph node involvement
Hepatosplenomegaly uncommon
˜ 25% of patients have extranodal disease only
Skin and soft tissue most common extranodal sites
Approximate frequency of extranodal sites
Skin and soft tissue (16%)
Nasal cavity and paranasal sinuses (16%)
Eye, orbit, and ocular adnexa (11%)
Bone (11%)
Salivary gland (7%)
Central nervous system (7%)
Oral cavity (4%)
Kidney and genitourinary tract (3%)
Respiratory tract (3%)
Liver (1%)
Tonsil (1%)
Breast (< 1%)
Gastrointestinal tract (< 1%)
Heart (< 1%)
Simultaneous involvement of multiple extranodal sites not unusual
Involvement of kidney, lower respiratory tract, and liver associated with worse clinical outcome (as is number of extranodal sites)
Treatment
Most patients require little intervention
Prognosis
Most patients have complete and spontaneous remission
Some may experience recurrent or persistent but stable lymphadenopathy
In very few cases, disease follows aggressive course and may be fatal
Poor prognosis correlates with widespread dissemination, involvement of kidneys, lower respiratory tract, and liver, and immunologic abnormalities or anemia
MACROSCOPIC FEATURES
General Features
In soft tissues and other extranodal sites
Firm, poorly marginated lesion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


