Right Hepatic Trisegmentectomy
Ivan R. Zendejas
DEFINITION
Removal of all the liver located to the right of the falciform ligament; the left lateral segment represents the functional remnant. By the segmental anatomy of the liver (FIG 1), this represents the resection of the three liver segments located to the right of the falciform ligament including the middle segment (4A and 4B), the right anterior segment (5 and 8), and the right posterior segment (6 and 7).
The resection may also include the caudate lobe and all the biliary ducts to the right of the umbilical fissure. This is most frequently indicated in hilar cholangiocarcinoma patients.
DIFFERENTIAL DIAGNOSIS
Cholangiocarcinoma
Metastatic carcinoma
Hepatocellular carcinoma
Gallbladder cancer
Liver trauma
PATIENT HISTORY AND PHYSICAL FINDINGS
Attention must be given to the potential for underlying liver disease. The intended hepatic remnant following right trisegmentectomy is inadequate.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Triphasic, contrast-enhanced abdominal computed tomography (CT) scan
Its main value is to identify the vascular structures involved, anatomic variations in the hilar vasculature, and margins to be preserved at the time of surgery (FIG 2).
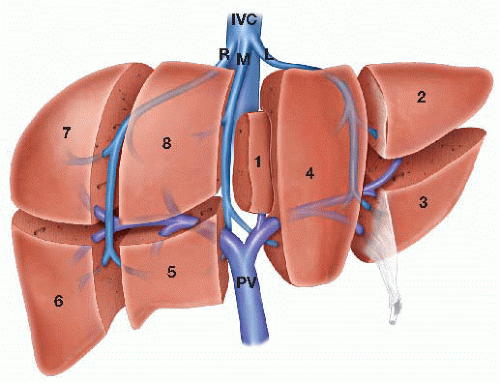
FIG 1 • Anatomy of a right trisegmentectomy. Segments 7 and 8 are routinely removed. Segment 1 is selectively included in the resection, depending on the indication and ability to obtain a negative resection margin.
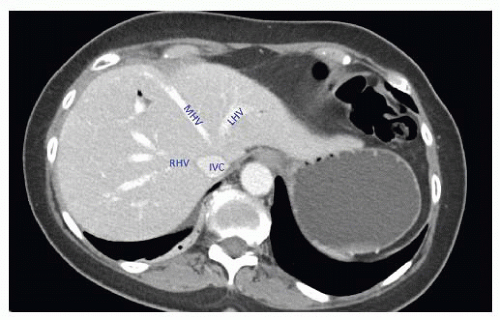
FIG 2 • Anatomy of the hepatic veins. The transection plane for a right trisegmentectomy is between the middle hepatic vein (MHV) and left hepatic vein (LHV).
Abdominal magnetic resonance imaging (MRI) with contrast and delayed liver phase
Equivalent to a contrast CT scan; slightly better at defining parenchyma abnormalities and in differential diagnosis
Intraoperative ultrasound (IOUS)
SURGICAL MANAGEMENT
Preoperative Planning
The volume of the intended remnant liver should to be calculated with preoperative imaging and considered against the patient body weight. The author favors 3-D reconstruction of a CT scan with software rendition of the remnant volume (FIG 7).
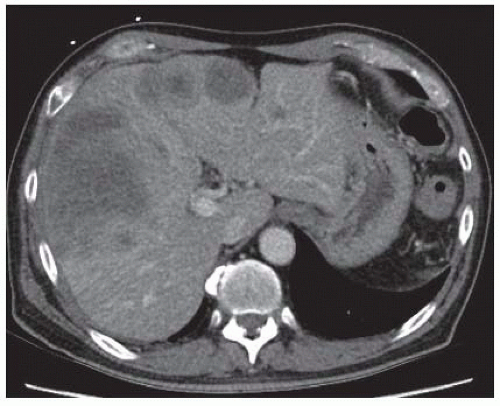
FIG 3 • Hepatocellular carcinoma involving the right and middle sectors.
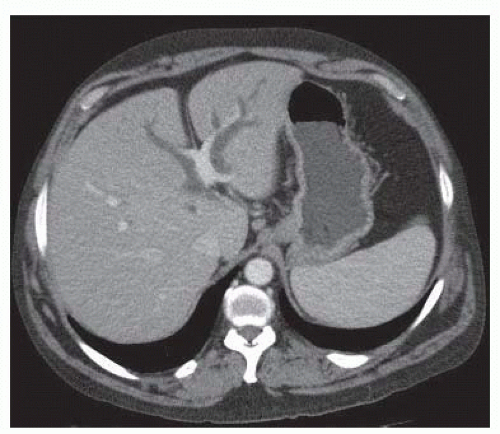
FIG 4 • Right dominant hilar cholangiocarcinoma. Note the dilated bile ducts in segment 4, to the right of the falciform ligament, suggesting the obstruction is distal to their confluence with the other ducts draining the left lobe.
The functional capacity of the remnant liver should be estimated.
Portal vein (PV) embolization of the right lobe (and occasionally segment 4) is often indicated.
If PV embolization is performed, CT scan volumetrics are repeated 3 to 4 weeks postembolization to assess for adequate hypertrophy of the planned liver remnant.
Low-volume intraoperative resuscitation reduces blood loss. This approach requires preoperative communication with the preoperative nursing staff and anesthesiologist.
Regional anesthesia approaches, such as epidural catheters, reduce pain scores and respiratory complications.
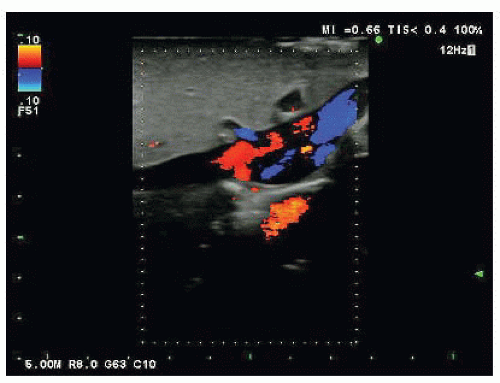
FIG 5 • Hepatic vein confluence under IOUS. Fluid-filled structures appear black. Doppler color facilitates identification of cystic lesions from vascular structures. In this image, the left hepatic vein is highlighted by the Doppler signal (blue) and the right hepatic vein is highlighted red as they insert into the inferior vena cava (IVC). The middle hepatic vein in this patient does not fuse with the left hepatic vein prior to IVC insertion and is seen above the IVC without Doppler enhancement.
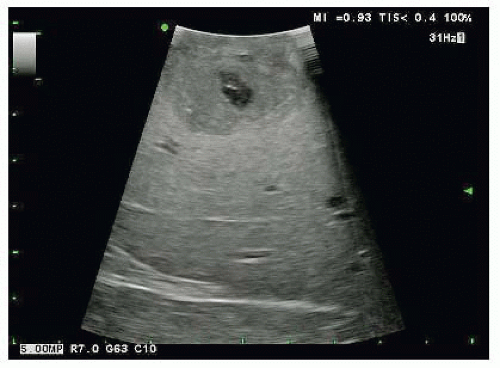
FIG 6 • IOUS of a hepatic neoplasm. The hypoechoic lesion is at the top of the image. The interface with normal parenchyma is readily apparent.
Preoperative steroid (100 mg intravenous [IV] methylprednisolone) is associated with reduced peaks of liver injury test values but not improved outcomes.
Positioning
The patient is placed in a supine position. Tucking the right arm is optional, depending on the retractor to be used.
The patient is prepped from the nipples to the pubis on both sides.
The authors routinely place an arterial line and central venous line.
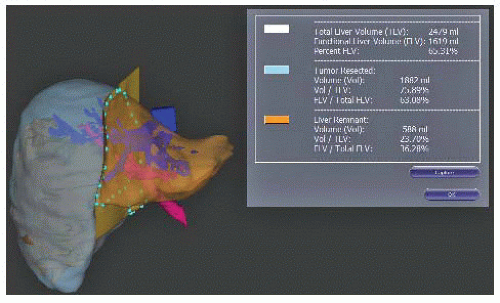 FIG 7 • Tridimensional reconstructions showing the volume of the liver remnant. This particular software package provides the volume and percent of the total volume (table insert). |
TECHNIQUES



