9 Rheumatological disease
Approach to the patient
Clinical features in musculoskeletal assessment
Drugs in rheumatology
Non-steroidal anti-inflammatory drugs (NSAIDs) (Table 9.1)
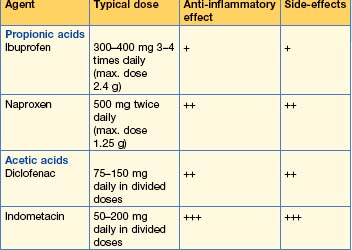
NSAIDs are inhibitors of both cyclo-oxygenase 1 and 2 isoenzymes and thereby inhibit the prostaglandin pathway (Fig. 9.1). Typical agents used for rheumatological disorders are shown in Table 9.1, although there are many others.
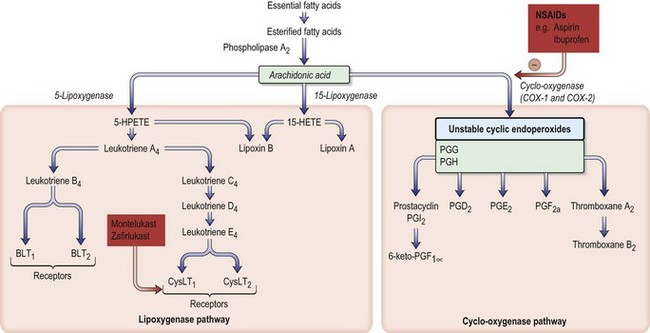
Fig. 9.1 Arachidonic acid metabolism and the effect of drugs. The sites of action of NSAIDs (e.g. aspirin, ibuprofen) are shown. The enzyme cyclo-oxygenase occurs in three isoforms: COX-1 (constitutive), COX-2 (inducible) and COX-3 (in brain). BLT, B leukotriene receptor; cysLT, cysteinyl leukotriene receptor; PG, prostaglandin.
NSAID should be used for the shortest possible time at the lowest effective dose.
Glucocorticoids
Systemic corticosteroids
These are potent anti-inflammatory agents.
Joint aspiration and injection for diagnosis and therapy (Box 9.3)
Aspiration
Aspiration should always be performed in patients with unexplained large joint effusions to obtain a diagnosis; for symptomatic relief in a patient with known arthritis; and to monitor response to treatment in an infected joint.
Box 9.3 Joint aspiration
This is a sterile procedure, which should be carried out in a clean environment.
Explain the procedure to the patient; obtain consent.
Joint injection
N.B. No more than three injections per joint should be performed in 1 year.
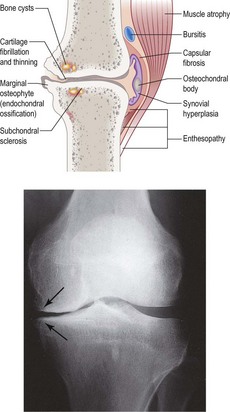
Osteoarthritis (OA)
Investigations
Management
Inflammatory arthritis
Rheumatoid arthritis (RA)
Clinical features

Investigations
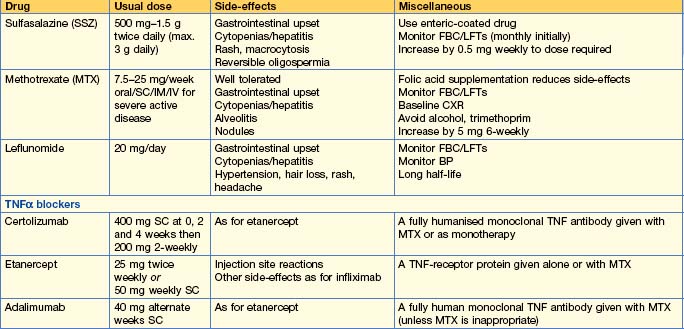
Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


