3 Respiratory system
After reading this chapter, you will:
Basic concepts
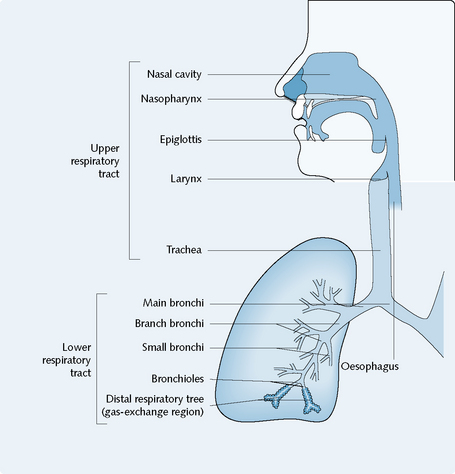
Respiration is the process of exchange of oxygen and carbon dioxide between an organism and its external environment. This principally involves the lungs, which possess the largest surface area in the body in contact with the external environment. The respiratory system (Fig. 3.1) has defence mechanisms which can be divided into physical (such as coughing or the mucociliary escalator, to remove foreign agents) and immunological (such as enzymes, pulmonary macrophages and lymphoid tissue, to ‘disarm’ foreign agents). These defence mechanisms can be launched inappropriately or may be insufficient to deal with the triggering agent, and thus disease may occur.
Obstructive airways diseases
Asthma
The stimuli cause asthmatic changes through several complex pathways (Fig. 3.2). The possible mechanisms of these pathways include the following:
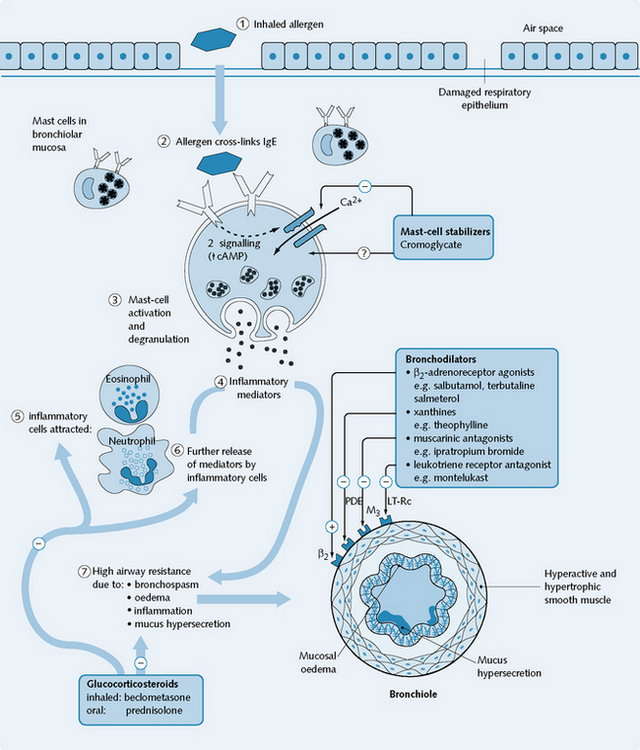
Late-phase response
Several hours later, the late-phase response occurs. This consists of bronchospasm, vasodilatation, oedema and mucus secretion caused by inflammatory mediators released from eosinophils, platelets and other cells, and neuropeptides released by axon reflexes. Anti-inflammatory drug action is necessary for the prevention and/or treatment of this phase (Fig. 3.2).
Management of obstructive airways disease
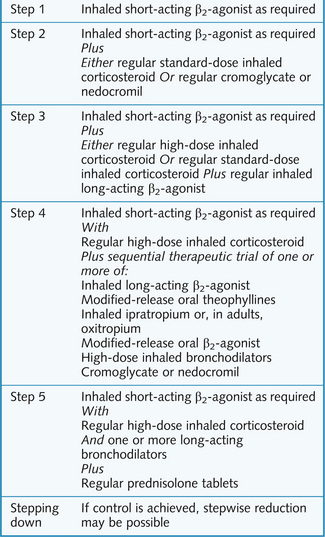
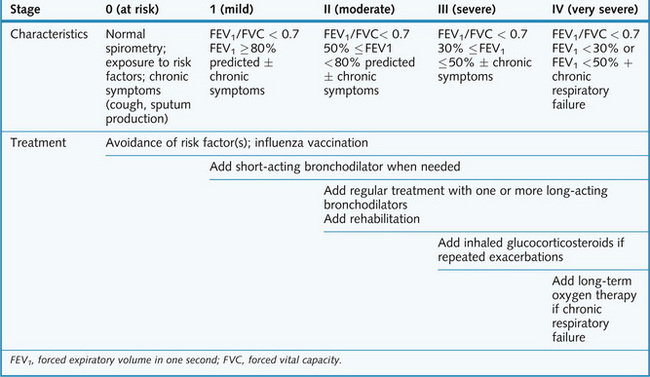
Anti-asthmatic drugs include symptomatic bronchodilators (these are most effective in the immediate-phase response), and prophylactic or anti-inflammatory agents, which prevent and/or resolve the late-phase response. The step-wise management of asthma is summarized in Figure 3.3; the stage-dependent treatment of COPD is shown in Figure 3.4. Most patients with COPD get some symptom relief from bronchodilators and anti-inflammatory agents in a fashion similar to people with asthma, yet the response of their airways to these drugs is much less marked, and there are no proved benefits for life expectancy. Long-term oxygen therapy does prolong survival in patients with COPD; however, this must be undertaken with care in patients with carbon dioxide retention because it will reduce their hypoxic drive to breathe.