Renal Artery Stenosis
A. Brad Farris, III, MD
Key Facts
Etiology/Pathogenesis
Renal artery stenosis from variety of potential causes results in ischemic atrophy
Atherosclerosis with atheromatous plaques is one of the most important etiologies
Clinical Issues
Hypertension
Proteinuria
Renal dysfunction
Macroscopic Features
Kidneys small from ischemic atrophy
Microscopic Pathology
Focal segmental and global glomerulosclerosis (FSGS) can occur
Glomerular basement membrane (GBM) wrinkling
Interstitial fibrosis and tubular atrophy (IFTA) and interstitial inflammation
Tubular atrophy is of conventional type or may show “endocrine change” or thyroidization
Atherosclerosis, arteriosclerosis, arteriolar hyalinosis, and sometimes cholesterol emboli
Electron microscopy may show GBM wrinkling and collapse, foot process effacement, and renin granules in hypertrophic juxtaglomerular apparatus
Top Differential Diagnoses
Renal artery aneurysms and dissection of aorta or renal artery
Neurofibromatosis
Takayasu arteritis and other arteritides
Fibromuscular dysplasia
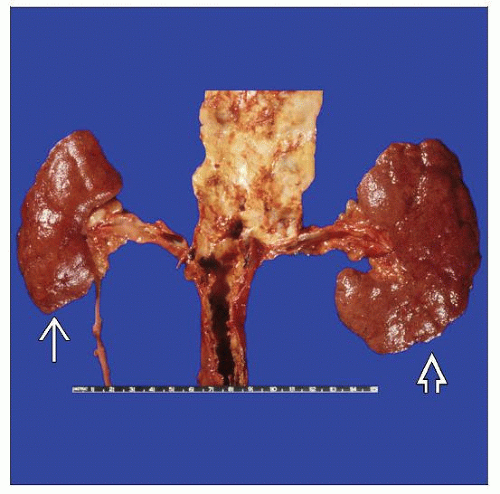 Shown here are a shrunken kidney  affected by renal artery stenosis and a granular kidney affected by renal artery stenosis and a granular kidney  affected by hypertension, likely stimulated by renin production by the shrunken kidney. affected by hypertension, likely stimulated by renin production by the shrunken kidney. |
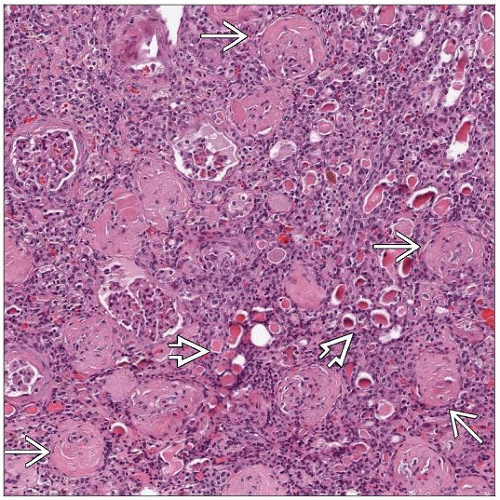 There are numerous sclerotic, closely approximated glomeruli  and tubular atrophy in a thyroidization pattern and tubular atrophy in a thyroidization pattern  in this kidney affected by renal artery stenosis. in this kidney affected by renal artery stenosis. |
TERMINOLOGY
Abbreviations
Renal artery stenosis (RAS)
Synonyms
Atherosclerotic renovascular disease: Certain cases of RAS
Fibromuscular dysplasia: Selected cases of RAS
Renovascular disease
Definitions
Narrowing of renal artery lumen sufficient to cause ischemic changes in kidney and hypertension
ETIOLOGY/PATHOGENESIS
Causes of RAS
Atherosclerosis
Most common cause of occlusion/stenosis of large renal arteries (70-90% of RAS cases)
Autopsy studies show RAS in 5-42% of patients
Up to 50% of patients with extensive peripheral vascular disease have RAS
RAS is bilateral in 33-39%
Bilateral RAS has higher incidence of renal failure
Patients often have multifocal occlusive vascular disease, including coronary artery disease or peripheral arterial disease
Injury is conceptually semiepisodic, leading to “layers” of injury with vessels that are not able to autoregulate, eventually leading to “critical stenosis”
Atheromatous plaques
More common with age and in those with risk factors (cigarette smoking, HTN, diabetes, hyperlipidemia)
Atheroemboli (cholesterol emboli)
May occur immediately after or within months of angiographic or surgical procedures involving vessels
0.1-0.8% frequency of symptomatic cholesterol emboli after angiography
Incidence of 0.1-3.3% in renal vessels
Emboli present in ˜ 31% of patients with aortic aneurysms and ˜ 77% of patients dying shortly after abdominal aortic surgery
Thromboembolic
Fibromuscular dysplasia
Neurofibromatosis
Moyamoya disease
Takayasu arteritis and other arteritides
Dissecting aneurysms of either aorta or renal artery
Umbilical artery catheterization in neonates
Coarctation of the aorta
Irradiation
Retroperitoneal fibrosis
Compression by tumor
Arteriovenous fistula
Trauma
Ischemic Renal Disease/Ischemic Nephropathy
Fundamental mechanism of injury in RAS
Occurs when renal artery has 70-80% or greater stenosis
Goldblatt Kidney
Unilateral RAS experimental model developed by Goldblatt has revealed pathophysiology
Causes hypertension (HTN) by activation of renal-angiotensin-aldosterone system
Ischemic kidney produces renin
Increased angiotensin II
Increased aldosterone production is stimulated
Leads to volume retention, hypervolemia, and increased cardiac output
Systemic HTN results
Ischemic kidney is protected from effects of HTN
Contralateral kidney suffers from effects of HTN (arterial and arteriolar nephrosclerosis)
CLINICAL ISSUES
Epidemiology
Age
Atherosclerotic RAS primarily affects older patients
Gender
2:1 male to female ratio in atherosclerotic RAS
Presentation
Renal dysfunction
Chronic renal insufficiency
Increased serum creatinine and blood urea nitrogen
Hypertension
Proteinuria
Usually of low or moderate degree
Particularly occurs in patients with focal segmental glomerulosclerosis (FSGS)
Retinopathy
Abdominal or flank bruits
Hypokalemia may sometimes be seen
Family history of HTN may be absent
Hyperlipidemia, particularly in patients with atherosclerotic RAS
Diabetes
Congestive heart failure
If atheroemboli are associated with RAS
Livedo reticularis
Acute renal failure
HTN
Leg pain
Gastrointestinal symptoms
Vision loss
Peripheral eosinophilia
Decreased serum complement
Treatment
Surgical approaches
Percutaneous transluminal angioplasty
Used more often than stent placement
Angioplasty
Can be coupled with stent placement
Particularly useful when stenosis is at renal artery ostium, where angioplasty has higher failure rate
Bypass grafts
Drugs
Antihypertensive agents
ACE inhibitors
Beta blockers
Calcium channel blockers
Lipid lowering agents
Antidiabetic agents and glucose control
Prognosis
With 70-80% narrowing of renal artery lumen, ischemic renal disease may occur and may rapidly progress to failure of affected kidney
Around 1/2 progress within 2 years
IMAGE FINDINGS
Radiographic Findings
Intraarterial digital subtraction is “gold standard” to demonstrate RAS
Other radiographic imaging modalities are useful
Magnetic resonance angiography
Computed tomographic angiography
Color-aided duplex ultrasonography
Abdominal aortography
If renal artery narrowing, there may be poststenotic dilatation
Radiography coupled with renal functional measurements are useful in determining contribution of each kidney to overall renal functioning
MACROSCOPIC FEATURES
General Features
Grossly, narrowing of renal artery may be appreciated
Origin from aorta involved in approximately 50% of cases
Aorta may override renal artery ostium
Bilateral disease in up to 60% of cases
Can occur from a yellow-white fibroatheromatous plaque (atheroma) in atherosclerotic RAS cases
Kidneys may be small in ischemic nephropathy from RAS
Most RAS kidneys are < 50% of normal weight
Large cortical scars and small cortical cysts may be present
Granular capsular surface is often evident because of concurrent arteriolosclerosis
Renal cortex is thinned
Interlobar and arcuate arteries may appear prominent
MICROSCOPIC PATHOLOGY
Histologic Features
Glomeruli
Glomeruli may have basement membrane wrinkling
Sometimes referred to as an accordion-like wrinkling
Particularly appreciable on periodic acid-Schiff (PAS) and silver stains
Glomerular capillary tuft may contract toward vascular pole (a process referred to as glomerulus becoming “simplified”), leading to relative increase in Bowman space
Intracapsular fibrosis
Collagen deposition in Bowman space
Occurs 1st near vascular pole, eventually extending toward urinary pole
“Atubular glomeruli” may be present
Typically are present as residual glomeruli in fibrotic scars
Open capillary loops are not attached to tubules on serial sectioning, and mean glomerular volume tends to be larger than in controls
FSGS with resultant global sclerosis can occur
FSGS occurs as secondary form
Proteinuria may be prominent
Juxtaglomerular apparatus may be hypertrophic
Tubulointerstitium
Interstitial fibrosis and tubular atrophy (IFTA), and interstitial inflammation
Fibrosis may be diffuse and fine, demonstrable with connective tissue stains (e.g., trichrome)
Interstitial fibrosis and inflammation may be more severe in hypertensive nephrosclerosis than in RAS
Dilated tubules (“super tubules”)
“Classic” atrophic proximal tubules
Thickened tubular basement membranes, possibly due to regeneration from repeated tubular injury
Numerous mitochondria with decrease in other cellular organelles
“Endocrine change” form of atrophic tubules
Decreased tubular diameter with narrowed or inconspicuous lumens
Cuboidal epithelial cell lining, often with clear cytoplasm
Often occur in clusters
Terminology derived from resemblance of these renal tubules to endocrine glands such as parathyroid
Thyroidization may also be seen, consisting of atrophic tubules filled with proteinaceous cast material
Tubular atrophy can be potentially reversible
Reversal of atrophy can be accomplished with reestablishment of blood flow in rat model of RAS
Atubular glomeruli may be useful prognostic sign (irreversible)
Vessels
Atherosclerosis
Important cause of renal artery stenosis
Eccentric thickening of intima with fibrosis, amorphous material including matrix proteins, lipid-laden macrophages (foam cells), and myofibroblasts
Cholesterol clefts may be seen, serving as potential source of cholesterol emboli that may be seen in renal parenchymal vessels
Medial fibrosis &/or thinning may be present, particularly where there is an overlying plaque
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


