FIGURE 24-1 Baseline 12-lead ECG. Sinus rhythm with unifocal PVCs in a pattern of bigeminy.
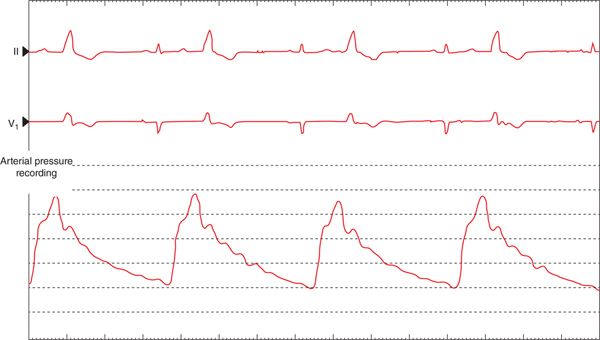
FIGURE 24-2 Arterial pressure recording during bigeminy. The absent cardiac output with the PVCs reflects the hemodynamic impact of frequent PVCs and that the effective heart rate is only about 35 bpm.
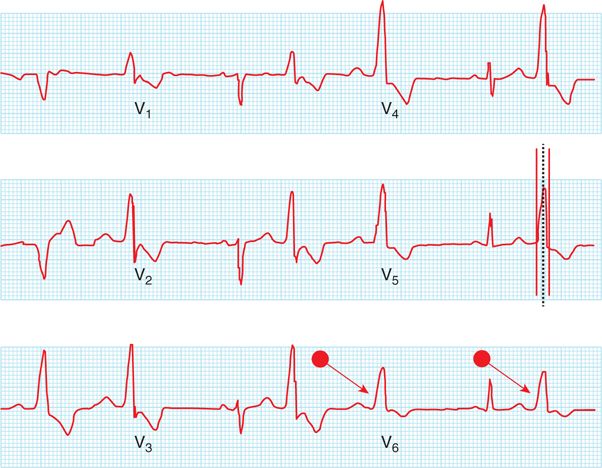
FIGURE 24-3 Assessment of maximal deflection index (MDI) and pseudo-delta wave. Duration of the PVC complex in V5 = 134 ms (red line to red line); duration of maximum deflection, V5 = 76 ms (first red line to dashed blue line), thus the maximum deflection index = 76/134 = .57. The pseudo-delta wave is denoted by red arrows in V6. The upstroke of the PVC is slowed, as if the activation is due to conduction over an accessory pathway, yet this ECG pattern is due to slow conduction when the ectopic beat originates from the epicardium and conducts toward the endocardium with late involvement of the His-Purkinje system.
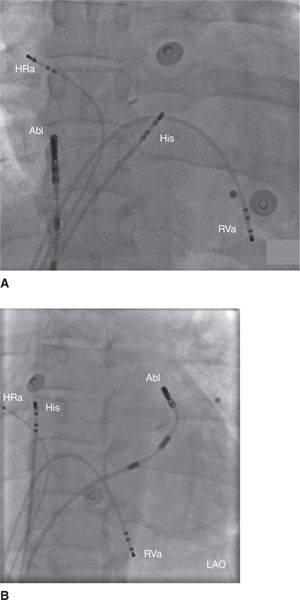
FIGURE 24-4 Fluoroscopic image of catheters during ablation procedure. HRa = quadripolar catheter in the high rate atrium catheter; Abl = magnetic-guided irrigated-tip ablation catheter; His = quadripolar catheter in the His position; RVa = quadripolar catheter in the right ventricular apex. (A) Anterior-posterior fluoroscopic image of the magnetic-guided irrigated-tip ablation catheter (Abl) in the right atrium. (B) Left anterior oblique (LAO) fluoroscopic image of the irrigated-tip ablation catheter (Abl), advanced using remote magnetic navigation, into the distal coronary sinus.
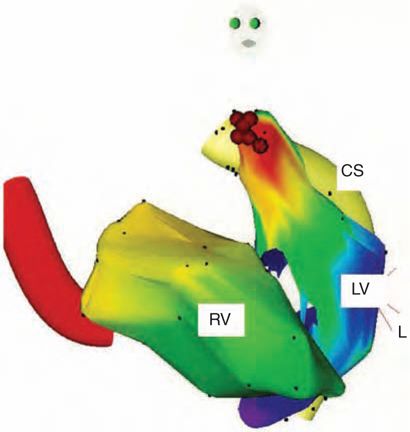
FIGURE 24-5 Pace-map of the PVC when pacing from the ablation catheter at the distal coronary sinus. Twelve-lead ECG: pace-mapping and spontaneous PVC from distal coronary sinus, 12/12 pace-map match.
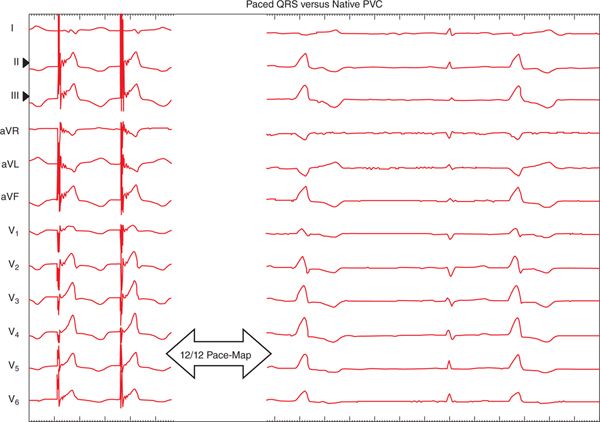
FIGURE 24-6 LAO image of electroanatomic map of PVC, including right ventricle (RV), left ventricle (LV), and the distal coronary sinus (CS). Successful ablation site of PVC denoted by red dots.
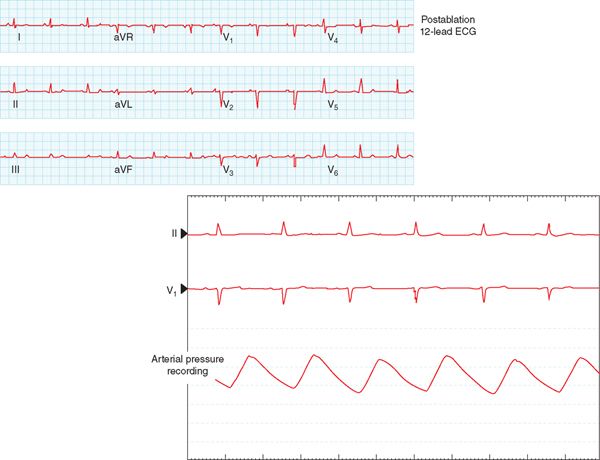
FIGURE 24-7 Immediately postablation, the 12-lead ECG shows sinus rhythm without PVCs (top) and the immediate hemodynamic improvement noted by the change in the arterial pressure line (bottom).
EPIDEMIOLOGY OF EPICARDIAL IDIOPATHIC PVCs
Diagnosis of idiopathic PVCs or ventricular tachycardia (VT) is feasible only after excluding structural heart disease. In the United States, 10% of VTs are idiopathic.5 The majority of patients with idiopathic PVCs will undergo electrophysiologic testing and attempt at radiofrequency ablation because of either symptomatic high burden PVCs with normal heart function,6 or ineffective antiarrhythmic therapy or tachycardia-induced cardiomyopathy,7 which has been reported to reverse by elimination of a high burden of PVCs.8
ELECTROCARDIOGRAPHIC CRITERIA OF IDIOPATHIC EPICARDIAL PVCs
Numerous studies have described the electrocardiographic features, pharmacologic intervention, and electrophysiologic mapping and ablation of epicardial PVC/VT.5,9–12 Electrocardiographic criteria of epicardial left ventricular origin include:
• Prolonged maximum deflection index (MDI) (Figure 24-3)—more than 0.55 is an important predictor of epicardial LVT arising from perivascular origin.1
• Pseudo-delta wave pattern noted with the PVC morphology (Figure 24-3)2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


