Reflux Nephropathy
Sanjay Jain, MD, PhD
Helen Liapis, MD
Key Facts
Terminology
Reflux nephropathy: Renal parenchymal scarring due to urine reflux
Etiology/Pathogenesis
Vesicoureteral reflux (VUR), UTIs
Exposure of kidneys to high-pressure urine reflux or bacteria causes tubulointerstitial damage and scarring
Intrarenal reflux in utero affects kidney development
Clinical Issues
Most common cause of severe hypertension in children
Manage UTIs, acute pyelonephritis, chronic pyelonephritis, and VUR
Diagnosis: DMSA scan; depends on adequate renal blood flow and cellular uptake
Prophylactic antibiotics and monitoring for nephropathy may be advisable for higher grades of reflux (4 and 5)
Microscopic Pathology
Tubulointerstitial inflammation, fibrosis, atrophy, and global glomerulosclerosis
Dysplasia indicates congenital component leading to reflux
Histological features in primary and secondary urine reflux may be similar and overlap with many features of obstructive nephropathy
Clinical and radiological correlation necessary
Top Differential Diagnoses
Obstructive nephropathy
Tubulointerstitial nephritis
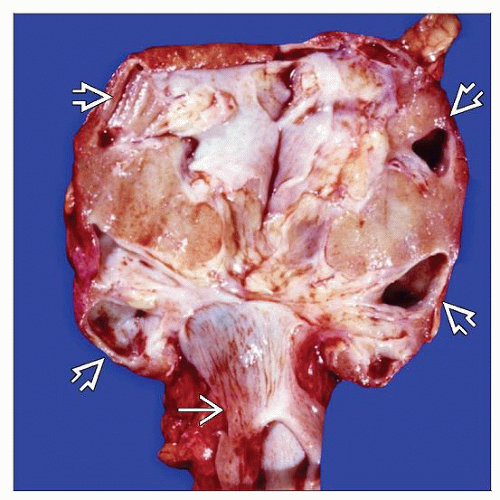 Reflux nephropathy with megaureter  shows marked thinning of the cortex and loss of the medulla, especially at the poles shows marked thinning of the cortex and loss of the medulla, especially at the poles  . . |
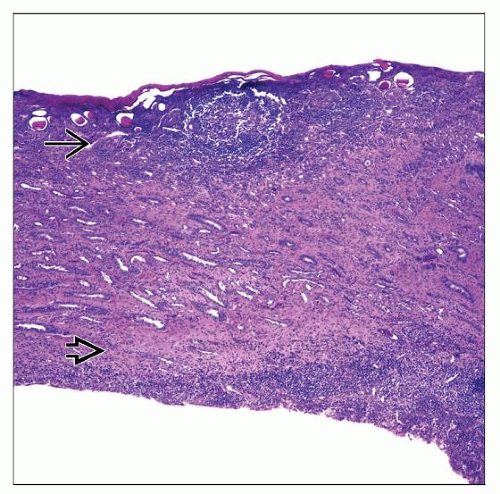 Cross-section through full-thickness of cortex  and medulla and medulla  in a 7-year-old boy with reflux nephropathy shows the markedly thin parenchyma corresponding to the gross appearance. in a 7-year-old boy with reflux nephropathy shows the markedly thin parenchyma corresponding to the gross appearance. |
TERMINOLOGY
Definitions
Reflux: Retrograde urine flow from bladder into ureters or kidney due to functional or physical lower tract defects
Reflux nephropathy: Renal parenchymal scarring due to urine reflux
ETIOLOGY/PATHOGENESIS
Causes
Vesicoureteral reflux (VUR)
Primary VUR
Congenital anomaly, unilateral or bilateral
Abnormal insertion of ureter into bladder, abnormal intravesicular tunnel length of ureter
Incompetent valve
Secondary VUR
Distal obstruction, neurogenic bladder: Posterior urethral valves (PUV), multiple sclerosis, spinal cord injury, stroke, diabetic neuropathy, pelvic surgery, B12 deficiency
Dysfunctional elimination syndrome: Abnormal holding of urine and voiding pattern
Acquired: Urinary tract infections
Pathophysiology Points
Reflux due to VUR or lower tract obstruction
Reflux nephropathy develops in some patients with VUR
Reflux urine enters renal parenchyma via compound papillae (2-3 fused papillae at poles that have round orifice)
Reflux gives bacteria access to kidney
Continued exposure of kidneys to high-pressure urine reflux or bacteria causes acute or chronic immune response
Tubulointerstitial damage ensues with these events leading to edema, ischemia, necrosis, inflammation, tubular atrophy, fibrosis, and scar formation
Focal scars in compound papillae
Ongoing damage can alter anatomy of simple papillae (dome-shaped with slit-like orifice and drain single lobe) to compound type and cause more diffuse scars
Glomerulosclerosis
Renin-angiotensin system is activated and causes hypertension
Etiology of scar formation is not fully understood
Reflux may not be a prerequisite for scar formation as scar can develop in kidneys without intrarenal reflux
Bacterial colonization of kidneys may not be necessary to induce kidney damage as scars have been observed in patients without history of urinary tract infection (UTI)
New renal scars can develop in presence of reflux and pyelonephritis
Intrarenal reflux during development can lead to partial or complete maturation and developmental arrest of developing kidney
Genes causing reflux may be similar to those important in kidney development
Genes tested and found to be associated with VUR phenotype in humans
HLA complex (DNA analysis and serotyping)
TNFα (DNA analysis)
TGFβ1 (DNA analysis)
ACE (DNA analysis, protein and mRNA studies)
PTGS2 (protein and mRNA studies)
IGF1 (protein and mRNA studies)
IGF1R (protein and mRNA studies)
EGF (protein and mRNA studies)
CCL2 (protein and mRNA studies)
ROBO2 (DNA analysis)
UPK3A (DNA analysis)
UPK1A (DNA analysis)
GNB3 (DNA analysis)
AGTR2 (DNA analysis)
ABO blood group (serotyping)
Finding of progression to kidney failure even after correction of reflux suggests ongoing irreversible damage
CLINICAL ISSUES
Epidemiology
Incidence
Reflux nephropathy is a cause of renal failure in 3-5% of renal dialysis or transplant patients
Most common cause of severe hypertension in children
Presentation
Hypertension
Proteinuria
UTI, acute pyelonephritis, chronic pyelonephritis
50-80% of children with febrile UTI have renal scarring
Primary or secondary VUR
Laboratory Tests
Renal parenchyma scintigraphy: Tc-99m dimercaptosuccinic acid (DMSA) scan; depends on adequate renal blood flow and cellular uptake
Voiding cystourethrogram (VCUG) for lower urinary tract disorder
Renal function test, urinalysis
Treatment
Surgical repair
Antibiotics
Prognosis
High-grade reflux more likely to cause nephropathy than low grade; 5% of renal failure in children due to reflux nephropathy
Proteinuria, reduced creatinine clearance and GFR, hypertension, high-grade reflux, and bilateral VUR increase likelihood of progression to chronic kidney disease
Management criteria are debatable; prophylactic antibiotics and monitoring for nephropathy may be advisable for higher grades of reflux (4 and 5)
Functional development of kidney may be affected if reflux in early embryogenesis
20% of renal failure in boys with reflux due to PUV
Urine Reflux Grading
5 grades depending on degree of anatomical changes in the collecting system due to reflux
Grade 1: Confined to ureter
Grade 2: Involves ureter and pelvis
Grade 3: More severe ureter and pelvis involvement with increased tortuosity
Grade 4: Grade 3 with blunting of calyces
Grade 5: Marked dilatation of pelvis and calyces, tortuosity of ureter
MACROSCOPIC FEATURES



