Problem 19 Rectal bleeding in a 45-year-old woman
A 45-year-old woman is referred with a 3-week history of rectal bleeding. She has noticed bright red blood on the toilet paper. The bleeding is associated with defaecation and is not mixed with the stool. Over the last 4 months she has suffered increasing constipation and tiredness. She has a good appetite, her diet has not altered recently, and her weight is stable. Her general health is good and she has had no major illnesses in the past. She describes troubles with ‘haemorrhoids’ since the birth of her chldren, and had some injection treatment for them. She smokes 10 cigarettes a day (and is trying to quit) and is not taking any medications.
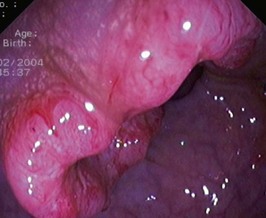
You explain to the patient that while the bleeding is most likely to be due to her haemorrhoids, a complete investigation of the large bowel is indicated. You arrange a colonoscopy. A lesion is found (Figure 19.1).
The patient wants to know if any of her children are at risk for developing this cancer.
You explain to the patient that the risk to her children is slightly greater than it would be for the general population. Table 19.1 shows the risks.
Table 19.1 Risk factors in colorectal cancer
| Family History | Risk |
|---|---|
| Up to 2 fold | |
| 3 to 6 fold | |
| 1 in 2 lifetime |
The son has heard that ‘polyps in the bowel usually turn to cancer’.
The patient remains in good health and is kept under regular surveillance.



