FIGURE 18-1 Shown is a 12-lead ECG with frequent PVCs in a bigeminal rhythm.
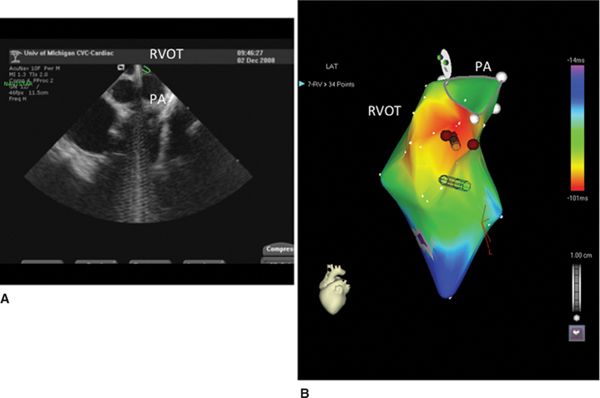
FIGURE 18-2 (A) Illustrates a view of the intracardiac echocardiogram with the ablation catheter located in the right ventricular outflow tract (RVOT; green icon) just below the pulmonary valve. (B) Illustrates an electroanatomic activation map of the RVOT from a left anterior oblique view. Brown tags indicate ablation lesions. The pulmonary annulus is marked (PA).

FIGURE 18-3 (A) Shown is the 12-lead ECG tracings and intracardiac recordings from the earliest endocardial site obtained during activation mapping of the PVC in the RVOT. (B) Shown is the 12-lead of the pace-map when pacing is performed from this location.
PVC MECHANISM
Triggered activity via delayed after depolarizations is the most likely mechanism of frequent PVCs, although reentry, especially in patients with structural heart disease and frequent PVCs, has been suggested as a possible mechanism as well.1 Reentry as a mechanism for PVCs has thus far only been demonstrated in animal models.2
PVC CARDIOMYOPATHY: AGGRAVATING FACTORS
Several features in this patient are associated with PVC cardiomyopathy. First, the PVC’s burden is >24%. This cut-off value best separated patients with PVC-induced cardiomyopathy from patients without PVC-mediated cardiomyopathy.3 Of note is that although based on ROC curves this cut-off value could be determined, not everyone with a PVC burden >24% had evidence of PVC-induced cardiomyopathy. About 25% of the patients with a higher PVC burden had normal left ventricular function. On the other hand, patients with a lower PVC burden were also at risk for PVC-induced cardiomyopathy, and the lowest PVC burden associated with PVC-induced cardiomyopathy was 10%.
By history, this patient’s PVCs were present for at least 10 years. Despite the fact that there is no documentation that the patient’s PVC burden was constant, data from Niwano et al suggest that a particular PVC burden often persists over several years.4 Multivariate analysis has recently demonstrated that a history of palpitations persisting more than 60 months was independently associated with PVC cardiomyopathy.5 In this study, the duration of palpitations was used as a surrogate for the amount of time a patient was exposed to PVCs.
Finally, this patient was asymptomatic, which appears to be another factor predisposing patients to PVC-induced cardiomyopathy.5 It is likely that asymptomatic patients seek medical attention later than symptomatic patients, thereby prolonging the exposure time to frequent PVCs.
PVC CARDIOMYOPATHY: NATURAL HISTORY
Not much data is available for the long-term natural history of patients with idiopathic PVCs, that is, in the absence of structural heart disease. In many prior reports where PVCs were associated with adverse outcome, the absence of structural heart disease was not well established.6 Niwano et al4 followed 239 patients without structural heart disease (confirmed by echocardiography and MRI) for at least 4 years. During follow-up, a decline in left ventricular function (>6%) was found in 13 patients. Most of these patients had very frequent PVCs that were defined as >20,000/24 hours in this study.
PVC CARDIOMYOPATHY: MECHANISM
The mechanism of PVC-induced cardiomyopathy is not known. Short-term animal research does not support fibrosis as a mechanism. This is supported by clinical studies confirming the absence of scar detected by MRI in patients with PVC-induced cardiomyopathy.7 A form of tachycardia-mediated cardiomyopathy is also unlikely, since the average heart rate in patients with PVC-induced cardiomyopathy is usually not different from patients with frequent PVCs without cardiomyopathy.8
PVC CARDIOMYOPATHY: THERAPY
PVC suppression by either medical therapy or ablation usually results in improvement and normalization of left ventricular function and dimensions.9,10 In the majority of patients, LV function normalizes within 4 months after an effective ablation, but this case illustrates that the process can take a longer period of time,11 possibly depending on the length of exposure to frequent PVCs.
PVCs: MAPPING AND ABLATION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


