Pulmonary Thrombi and Emboli
Part 1 Thromboemboli
Abida K. Haque
Pulmonary thromboemboli may be massive, resulting in sudden death, or they may be smaller, with symptoms of mild respiratory distress. Large thromboemboli often originate in the deep leg veins and impact at the pulmonary artery bifurcation with complete occlusion, forming a “saddle embolus.”
Histologic Features
Thrombi show a laminated appearance, and the lines of Zahn are firm and granular.
Postmortem clots are soft and have two distinct components resembling red currant jelly and chicken fat.
Once lodged in the pulmonary artery, the thrombi show evidence of organization, with an initial neutrophilic response in the vessel wall, followed by neutrophil infiltration of the thromboembolus and then fibroblast ingrowth within approximately 1 week.
Thrombus is ultimately fibrosed and may be recanalized.
 Figure 55.1 Gross figure showing a pulmonary artery distended with an endoluminal thromboembolus. |
 Figure 55.2 Gross figure showing a pulmonary artery with a laminated, firm, granular thromboembolus. |
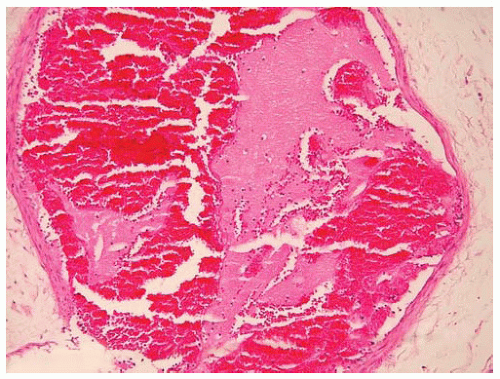 Figure 55.3 Small pulmonary artery distended with a recent thromboembolus, consisting mostly of fibrin and red blood cells. |
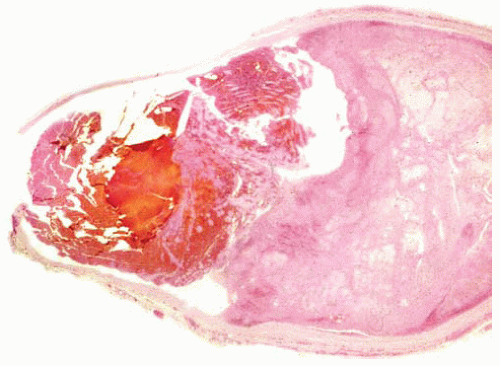 Figure 55.4 Organizing thromboembolus with lysed red blood cells suggesting a slightly less recent event. |
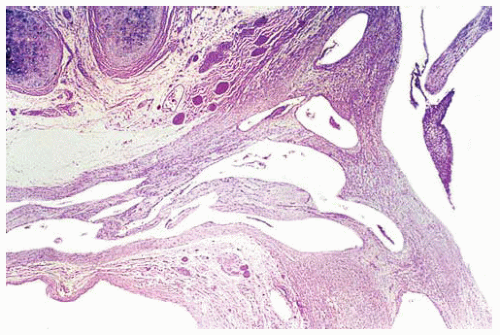 Figure 55.5 Large pulmonary artery branch with old organized thrombus replaced by pulmonary webs. |
Part 2 Foreign Body Emboli
Abida K. Haque
Intravenous entries of fragments of plastic catheters and tubings, cotton fibers, and rarely bullets have been reported. Diagnosis is based on gross observation and clinical history.
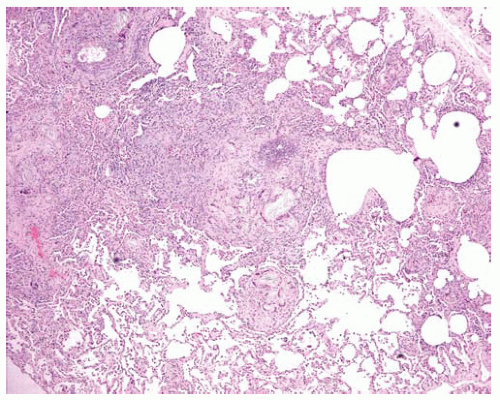 Figure 55.6 Multiple foreign-body giant-cell granulomas with multiple refractile plate-like crystals.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|