Figure 15G.1.1 Inoculation of a chicken egg with influenza virus.
6. Discard the syringe and needle into a sharps safety container.
7. Seal the hole punched in the eggshell with a drop of white glue.
Care should be taken not to contaminate glue in bottle with virus.
8. Incubate human influenza A virus for 48 hr at 33° to 37°C and influenza B viruses for 72 hr at 33° to 35°C.
Harvest virus from infected eggs
9. Chill eggs overnight (12 to 24 hr) at 4° to 8°C to halt embryo viability and minimize the flow of blood into the allantoic fluid during harvest.
Eggs may be quick-chilled for 30 min in a −20°C freezer. However, this may cause the allantoic fluid to contain some blood.
10. With sterile forceps, break the shell over the air sac and push aside the allantoic membrane with the forceps, taking care not to break the yolk.
If the allantoic fluid is mixed with the yolk, the fluid should be discarded.
11. Using a 10-ml pipet, aspirate the allantoic fluid and place in a labeled 50-ml conical tube. Dispose of eggs in an appropriate biological waste container.
12. Centrifuge the tubes 5 min at 500 × g, 4°C, to pellet any blood cells and tissue fragments. Transfer clarified fluid into fresh 50-ml tube. Keep on ice or at 4° to 8°C.
13. Perform a hemagglutination test (see Basic Protocol 3).
14. Dispense allantoic fluid into 2-ml aliquots in 2-ml sterile cryovials and store <1 year at −70° to −80°C or at −135° to −150°C for long-term storage (see Basic Protocol 3).
PROPAGATION OF INFLUENZA VIRUS IN EMBRYONATED CHICKEN EGGS FROM PRIMARY CLINICAL SPECIMENS
Original clinical material is inoculated into both the amniotic and allantoic cavities. Virus inoculated into the amniotic sac that surrounds the embryo can replicate directly in the embryonic tissue, and the resulting virus is released into the amniotic fluid. However, the amniotic sac will yield only a small volume of fluid, and thus subsequent passage into the allantoic cavity may be required to produce sufficient volume for testing.
Additional Materials (also see Basic Protocol 2)
Primary clinical specimen (see Support Protocol 3)
Egg candler (KUHL)
1. Dilute primary clinical specimen in egg diluent.
The concentration of the seed stock will determine how dilute the inoculum should be. Typically, an original specimen will be diluted 1:10 to achieve optimal virus growth.
2. Inoculate three eggs per specimen; label eggs to clearly identify original sample.
3. Punch a small hole in the shell over the air sac using an 18-G, 1/2-in. needle and dispose of needle in appropriate sharps container.
4. Aspirate 0.6 ml clinical specimen into a 1-ml syringe with a 21-G, 1/2-in. needle.
5. Using an egg candler apparatus, hold the egg up to light source and locate the embryo.
6. Insert the needle into the amniotic sac and inoculate 0.1 ml primary clinical specimen into the sac. Withdraw the needle carefully about 1/2-in. and inoculate 0.2 ml primary clinical specimen into the allantoic cavity (Fig. 15G.1.1).
7. Repeat with remaining clinical specimen and eggs.
8. Discard the syringe and needle into a sharps safety container.
9. Seal the holes punched in the egg shells with a drop of white glue.
Care should be taken not to contaminate glue in bottle with virus.
10. Incubate the eggs for 48 to 72 hr at 33° to 37°C.
The incubation temperature is dependent on the virus being grown (i.e., influenza A at 37°C and influenza B at 33°C).
11. Harvest the allantoic fluid as described in Basic Protocol 2, steps 9 through 11. Keep the tubes on ice (4° to 8°C).
12. Invert the egg so that the embryo and amniotic sac hang down and are clearly visible and separate from the egg yolk. Using a 1-ml syringe and 21-G, 1-in. needle, pierce the air sac and remove as much amniotic fluid as possible from around the embryo. Dispose of eggs in an appropriate biological waste container.
Keep allantoic and amniotic samples separate as the amniotic fluid may contain more virus than the allantoic fluid. The volume of allantoic fluid recovered may vary from 5 to 10 ml, while the volume of the amniotic fluid recovered may vary from 0.1 ml to 1 ml.
The amniotic cavity provides a richer source of susceptible cells for virus replication and is used to help viruses from primary specimens grow more efficiently.
13. Centrifuge the tubes 5 min at 500 × g, 4°C, to pellet any blood cells and tissue fragments. Transfer clarified fluid into a fresh tube. Keep the tubes on ice or at 4° to 8 C.
14. Perform a hemagglutination test on both the allantoic and amniotic fluids (see Basic Protocol 3).
If the hemagglutination test is negative or titer is <8 HAU, passage the specimen two more times before reporting inability to recover virus from the specimen. If HA test results in titers >8 HAU, specimens can be dispensed into aliquots and stored.
15. Dispense allantoic and amniotic fluid (if both have sufficient titers) into sterile 2-ml cryovials and store up to 1 year at −70° to −80°C or in liquid nitrogen at −135° to −150°C for optimal viability for long-term storage (see Basic Protocol 7).
QUANTIFICATION OF INFLUENZA VIRUSES BY HEMAGGLUTINATION ASSAY
Hemagglutination, or the ability to bind red blood cells, is a property of all influenza viruses that can be utilized as a rapid assay for determining the presence of virus in samples. The hemagglutination (HA) assay is dependent on the amount of hemagglutinin on the surface of influenza viruses and not the ability of the virus to replicate; this assay quantifies viral particles regardless of their infectivity. The highest dilution of virus that causes complete hemagglutination is considered the HA titration end point. The HA titer is the reciprocal of the dilution of virus in the last well with complete hemagglutination. A “unit” of hemagglutination is not a measure of an absolute amount of virus, but is an operational unit dependent on the method used for HA titration. An HA unit (HAU) is defined as the amount of virus needed to agglutinate an equal volume of a standardized red blood cell suspension. This protocol uses turkey red blood cells as an example, as these cells can be agglutinated by recent human influenza viruses as well as laboratory-adapted strains of human origin. Refer to Support Protocol 4 for a discussion of other types of red blood cells that can be used for hemagglutination assays. Hemagglutination units reflect either infectious or non-infectious influenza viruses, and thus can be used with inactivated influenza in experiments. For determining infectious units, use the 50% tissue culture infectious dose assay (see Basic Protocol 4), 50% egg infectious dose assay (see Basic Protocol 5), or the plaque assay (see Basic Protocol 6).
Standardized turkey red blood cells (see Support Protocol 4)
96-well V-shaped microtiter plate (Nunc)
NOTE: Keep the virus stock on ice or at 4° to 8°C during the HA test to maintain virus infectivity.
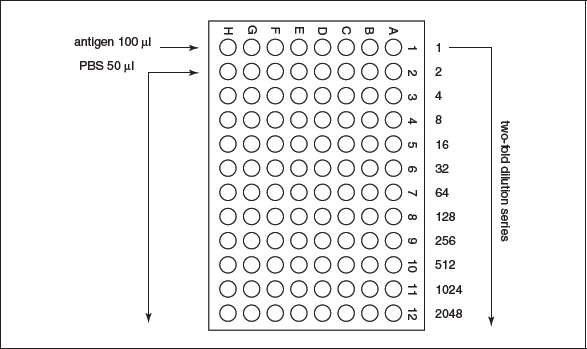
1. Pipet 50 µl PBS into wells 2 through 12 across a 96-well V-shaped microtiter plate (Fig. 15G.1.2).
Figure 15G.1.2 Plate layout for hemagglutination titration assay.
NOTE: 96-well V-shaped microtiter plates are used for avian red blood cells and U-shaped are used for mammalian red blood cells.
2. Pipet 100 µl influenza virus stock into the first column of the 96-well plate.
3. Perform a two-fold dilution series across the 96-well plate by transferring 50 µl between wells, mixing three to five times and disposing of the final 50 µl from the last well.
4. Add 50 µl standardized turkey red blood cells to all wells. Tap the plate or use a mechanical plate shaker to mix.
Approximately 5 ml of standardized turkey red blood cells is used per 96-well plate.
5. Incubate 96-well plate for 30 min at room temperature (24° to 27°C).
Avian red blood cells in V-shaped microtiter plates require 30-min incubation at room temperature, whereas mammalian red blood cells require a U-shaped microtiter plate with a 60-min incubation at room temperature.
6. Observe endpoint of agglutination and record titer per 50 µl of sample (Fig. 15G.1.3).
Figure 15G.1.3 Reading a hemagglutination titration assay plate. Positive samples will look pink as the red blood cells are held in solution by the virus. Negative samples will look clear with a red dot, since the red blood cells settle to the bottom of the V-bottom plate.
Red blood cells will settle to the bottom of the V-bottom well in negative samples, while red blood cells will agglutinate in positive samples. The endpoint should be read as the last well showing complete agglutination.
7. Store the virus stocks with desired HAU titers (see Alternate Protocol 14, step 14).
Dispose of materials in an appropriate biological waste container.
QUANTIFICATION OF INFLUENZA VIRUSES BY 50% TISSUE CULTURE INFECTIOUS DOSE ASSAY
The 50% tissue culture infectious dose (TCID50) assay is a method to measure the amount of infectious virus in a sample by determining the highest dilution of the sample that can infect 50% of cells in culture. In this procedure, the virus sample is diluted across a 96-well tissue culture plate containing MDCK cells. The titration should be performed in quadruplicate.
Materials
MDCK cells in 96-well tissue culture plate (see Support Protocol 1)
Influenza virus growth medium (see recipe)
Influenza virus stock
96-well tissue culture plate (Costar)
Inverted microscope
NOTE: All equipment and solutions coming into contact with cells must be sterile and proper sterile technique should be used accordingly.
NOTE: All culture incubations are performed in a 35° to 37°C, 5% CO2 humidified incubator.
1. Remove MDCK growth medium from the plate and wash the cells by adding 350 µl influenza virus growth medium to all wells. Aspirate the medium and repeat washing step. Care should be taken not to disrupt the cell monolayer.
2. Add 100 µl influenza virus growth medium to all wells, except the first column, of a 96-well tissue culture plate.
3. Thaw the influenza virus stock and dilute 1:100 in influenza virus growth medium.
4. Add 146 µl diluted virus to the first column of the 96-well tissue culture plate and perform a 1/2 log10 dilution series by transferring 46 µl from column to column, disposing of final 46 µl after the eleventh column. Do not add virus to the final column as this is the cell control for the assay.
5. Incubate the plates 2 hr at 35° to 37°C.
6. Remove the inoculum and gently wash once with 250 µl influenza virus growth medium.
7. Add 200 µl influenza virus growth medium to all wells and incubate up to 72 hr at 35° to 37°C, observing for endpoints in cytopathic effect (CPE).
Typical CPE by influenza viruses include rounding up of infected cells and detachment from culture flask.
8. Examine the wells for presence or absence of CPE using an inverted microscope.
To confirm results, 50 µl cell culture supernatant can be harvested into a 96-well V-bottom microtiter plate and tested for presence of virus by performing a spot HA assay (see Basic Protocol 5).
9. Record endpoint of CPE and determine TCID50 titer per 100 µl using the Reed-Muench method (see Support Protocol 5).
QUANTIFICATION OF INFLUENZA VIRUSES BY 50% EGG INFECTIOUS DOSE ASSAY
The 50% egg infectious dose (EID50) assay is a method to measure the amount of infectious virus in a sample by determining the highest dilution of the sample that can infect 50% of eggs. The EID50 assay entails performing serial dilutions. The Reed-Muench method is used to calculate the dilution that will produce a 50% positive result. The Reed-Muench method requires the use of three or more eggs per dilution to determine the 50% endpoint by performing a hemagglutination assay for each egg.
Materials
Egg diluent (see recipe)
Influenza virus stock
9- to 11-day-old embryonated chicken eggs (see Support Protocol 2)
Standardized turkey red blood cells (see Support Protocol 4)
1.5-ml microcentrifuge tubes, sterile
Forceps, sterile
96-well V-shaped microtiter plate (Nunc)
Additional reagents and equipment for inoculating eggs (see Basic Protocol 2)
NOTE: All equipment and solutions coming into contact with embryonated eggs must be sterile and proper sterile technique should be used accordingly.
1. Label ten 1.5-ml microcentrifuge tubes 1 through 10 and fill each with 450 µl egg diluent.
2. Pipet 50 µl influenza virus stock into 450 µl egg diluent in the first tube and perform a ten-fold dilution down to 10–10 by transferring 50 µl between tubes.
Changing tips between tubes will decrease the chance of sample carryover and will result in a more accurate titration of the virus.
3. Inoculate at least three eggs with 100 µl per dilution as described in Basic Protocol 2, steps 1 to 8.
4. Incubate the eggs for 48 to 72 hr at 33° to 37°C.
The incubation temperature and time is dependent on the virus being grown (i.e., influenza A at 37°C for 48 hr and influenza B at 33°C for 72 hr).
5. Chill the eggs overnight (12 to 24 hr) at 4° to 8°C to halt embryo viability and minimize the flow of blood into the allantoic fluid during harvest.
Eggs may be quick-chilled for 30 min in a −20°C freezer. However, this may cause the allantoic fluid to contain some blood.
6. With sterile forceps, break the shell over the air sac and push aside the allantoic membrane with the forceps.
7. Pipet 50 µl allantoic fluid from each egg to a corresponding well in a 96-well V-shaped plate.
Avian red blood cells in V-shaped microtiter plates require 30-min incubation at room temperature, whereas mammalian red blood cells require a U-shaped microtiter plate with a 60-min incubation time at room temperature.
8. Add 50 µl standardized turkey red blood cells to all wells and incubate 30 min at room temperature (24° to 27°C).
One 96-well plate requires ∼5 ml standardized turkey red blood cells
9. Observe endpoint of agglutination and record.
Red blood cells will settle to the bottom of the V-bottom well in negative samples, while red blood cells will agglutinate in positive samples. The endpoint should be read as the last well showing complete agglutination.
10. Determine the EID50 titer per 100 µl by the Reed-Muench method (see Support Protocol 5).
QUANTIFICATION OF INFLUENZA VIRUSES BY PLAQUE ASSAY
Influenza viruses cause cytopathic effect (CPE) and death of the infected cells leading to the formation of plaques or circular zones of lysed cells on a monolayer. Only infectious virus particles should infect the host cell and be able to produce a plaque. The plaque assay is a method to measure the amount of infectious virus in a sample by determining the number of plaque forming units on a cell monolayer, typically MDCK cells. At a high dilution of virus stock, each plaque represents the zone of cells infected by a single virus particle. Therefore, the titer of a virus stock can be calculated in plaque forming units per milliliter. The titration should be carried out in duplicate.
Materials
2× plaque assay medium (see recipe)
1.6% (w/v) agarose solution
Influenza virus stock
Madin-Darby canine kidney (MDCK) cells confluent in 6-well tissue culture plates (see Support Protocol 1)
Plaque assay wash medium (see recipe)
2 mg/ml TPCK-trypsin working stock (see recipe)
70% ethanol
0.3% crystal violet solution
37° and 56°C water baths
Forceps, sterile
Inverted microscope
NOTE: All equipment and solutions coming into contact with cells must be sterile and proper sterile technique should be used accordingly.
Prepare the media and stock
1. Before beginning the plaque assay, warm 2× plaque assay medium in a 37°C water bath and place 1.6% agarose solution in a 56°C water bath.
The 2× plaque assay medium should be warm enough so as not to solidify the 1.6% agarose solution when mixed together; also it should not be too hot, which will kill the MDCK cell monolayer when the media solution is added. The 1.6% agarose solution should be kept at 56°C to keep the solution from solidifying before use. When both solutions are mixed together the temperature of the resulting solution should be suitable for immediate addition to the MDCK cell monolayer while maintaining cell viability.
2. Thaw a vial of influenza virus stock in cool water.
Keep the virus on ice or at 4° to 8°C once thawed to reduce loss of infectivity.
Infect the cells in the 6-well tissue culture plates
3. Remove the MDCK growth medium from the 6-well tissue culture plates and wash the MDCK monolayer three times with room temperature plaque assay wash medium.
For wash steps, either a sterile 10-ml pipet or 1000-µl pipettor may be used to remove and add the medium. Do not pipet medium directly onto the monolayer as this may disrupt the cells.
Fetal bovine serum (FBS) inhibits viral entry and must be removed for efficient infection of cells.
4. Perform a ten-fold dilution series starting at 10–1 and diluting virus samples down to 10–10 in plaque assay wash medium. Change disposable pipet or pipet tips between tubes to decrease the chance of sample carryover.
Only gold members can continue reading. Log In or Register to continue