Proctoscopy
This chapter deals with the performance of rigid proctoscopy (sometimes called rigid sigmoidoscopy). Flexible fiberoptic sigmoidoscopy is performed essentially as detailed in Chapter 96, except that the distance to be traversed is not as great. Rigid proctoscopy is indicated in patients who have poorly prepped colons or who are being examined for foreign bodies or massive lower gastrointestinal bleeding. In these cases, the fiberoptic scope may not permit an adequate examination. The figures in this chapter detail the sequence of maneuvers necessary to pass the rigid proctoscope and to examine the rectosigmoid colon thoroughly.
SCORE™, the Surgical Council on Resident Education, classified proctoscopy as an “ESSENTIAL COMMON” procedure.
STEPS IN PROCEDURE
Left lateral decubitus or prone jackknife position (knee–chest position)
Digital rectal examination
Gently introduce scope with obturator in place
Anal canal angles forward, then directly back
Remove obturator when sphincters have been crossed
Use gently insufflation to open the lumen
Pass the scope under direct vision
Angle the scope from side to side to traverse the rectal valves
At about 15 cm, an angulation at the peritoneal reflection will be encountered
Do not pass the scope beyond this point unless it goes easily under direct vision
HALLMARK ANATOMIC PROCEDURES
Perforation
Missed lesion
LIST OF STRUCTURES
Anal canal
Rectum
Sigmoid colon
Peritoneal reflection
Rectal valves (of Houston)
Positioning of the Patient and Insertion of the Scope (Fig. 125.1)
Technical Points
Place the patient on a proctoscopy table in the knee–chest position. If such a table is not available, the left lateral decubitus or Sims position is a useful alternative. If the patient is in the Sims position, make sure that the buttocks extend over the edge of the table. This will allow you to maneuver the scope fully and to move your head around as needed to get a good view of the entire lower bowel.
First, perform a digital rectal examination to confirm that there is no pathologic lesion within the immediate anorectal
area and to determine the angle of the rectal canal. Place the obturator within the proctoscope and introduce the scope by gentle pressure.
area and to determine the angle of the rectal canal. Place the obturator within the proctoscope and introduce the scope by gentle pressure.
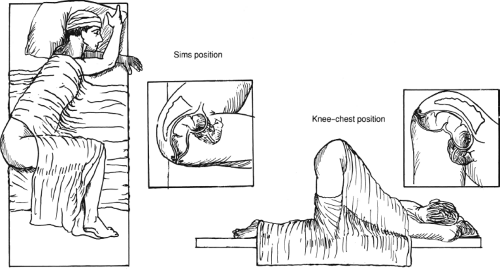 Figure 125.1 Positioning of the patient and insertion of the scope |
The anal canal first passes anteriorly and then angles sharply back toward the hollow of the sacrum. Therefore, the scope must initially be passed in a direction pointing toward the patient’s umbilicus, and then almost immediately angled back toward the small of the back after the sphincter mechanism has been traversed. As soon as you feel the scope traverse the sphincter mechanism, remove the obturator and pass the scope under direct vision. On the way in, concentrate on passing the scope safely and atraumatically. On the way out, concentrate on visualizing and examining the entire rectosigmoid colon for any signs of pathology.
The first few centimeters of the scope in the lower rectum should take you straight back toward the hollow of the sacrum. It will then be necessary to pass the scope more anteriorly. Insufflate air as you proceed in order to open up the bowel enough to see where you are headed. Angle the scope from side to side to traverse the rectal valves (of Houston), of which there are generally three. When you have inserted the scope to a depth of about 15 cm, you will have reached the peritoneal reflection and the bowel will angle sharply, usually to the left. At this point, you must angle the tip of the scope sharply to pass by it. Often, it is not possible to pass the scope deeper than 15 to 18 cm. If you cannot advance it safely under direct vision, do not attempt to do so.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


