Abdominal Aortic Aneurysm Repair and Aortofemoral Bypass
Lilja Thyri Bjornsdottir
W. John Sharp
Many aortic aneurysms are now repaired by an endovascular route. The classic open operation is still required in some circumstances. In this chapter, the anatomy of the abdominal aorta and iliac vessels is explored through the procedure of abdominal aortic aneurysm repair. The femoral region is then introduced through the closely related procedure of aortofemoral bypass grafting.
SCORE™, the Surgical Council on Resident Education, classified abdominal aortic aneurysm repair (open) and aortofemoral bypass as “ESSENTIAL UNCOMMON” procedures.
STEPS IN PROCEDURE
Abdominal Aortic Aneurysm Repair—Transperitoneal Approach
Midline incision from xiphoid to below umbilicus
Reflect transverse colon cephalad
Reflect duodenum and small bowel cephalad and to the right
Retract descending colon and sigmoid to the left
Preclot graft, if necessary
Isolate proximal and distal neck of aneurysm in preparation for clamping
Heparinize patient
Clamp aorta proximally and distally
Open the anterior wall of the aneurysm (longitudinal incision, T-ed across at superior and inferior ends)
Remove mural thrombus and suture-ligate any back-bleeding lumbar vessels
Suture-ligate the inferior mesenteric artery (from inside the aneurysm wall) if it is back bleeding
Anastomose graft to proximal aorta using running suture
Flush and then clamp the graft distally; inspect suture line for leaks
Complete distal anastomosis and flush before opening clamps
Close the aneurysm sac over the graft after obtaining hemostasis
Abdominal Aortic Aneurysm Repair—Retroperitoneal Approach
Supine position with chest in right lateral decubitus position
Incision from the tip of eleventh rib to midhypogastrium
Divide all muscular and fascial layers in the direction of the incision (not their fibers)
Mobilize the peritoneal sac medially to expose the aorta and both iliac vessels
Proceed as outlined above
Aortobifemoral Bypass
Expose femoral vessels by incision over each femoral pulse (inguinal ligament downward for approximately 10 cm)
Isolate and control the femoral arteries and branches
Create retroperitoneal tunnels over the anterior surface of the iliac and femoral arteries
Midline incision and exposure of the aorta as outlined above
Place clamp on proximal aorta, taking care not to fracture plaque
Clamp common, superficial, and profunda femoris arteries
Anastomosis to aorta can be performed as end (aorta)-to-end (graft) or as side (aorta)-to-end (graft)
Anastomosis to femoral vessels is end (graft)-to-side (vessel)
Obtain hemostasis and close
HALLMARK ANATOMIC COMPLICATIONS
Left colonic ischemia from inadequate collaterals
Injury to ureters
Injury to left renal vein
Injury to hypogastric nerve plexus
Seroma (lymphocele) formation in groin incisions
LIST OF STRUCTURES
Aorta
Left and right renal arteries
Left and right gonadal arteries
Inferior mesenteric artery
Lumbar arteries
Left and right common iliac arteries
Left and right internal iliac (hypogastric) arteries
Left and right external iliac arteries
Left and right common femoral arteries
Superficial circumflex iliac artery
Superficial epigastric artery
Superficial external pudendal artery
Profunda femoris artery
Medial femoral circumflex artery
Lateral femoral circumflex artery
Inferior Vena Cava
Left renal vein
Left and right common iliac veins
Left and right internal iliac veins
Left and right external iliac veins
Femoral vein
Profunda femoris vein
Hypogastric nerve plexus
Duodenum
Ligament of Treitz (suspensory muscle of the duodenum)
Ureters
External oblique muscle
Internal oblique muscle
Transversus abdominis muscle
Anterior rectus sheath
Rectus abdominis muscle
Inguinal ligament
Femoral sheath
Femoral triangle
Femoral Nerve
Cutaneous branch
Muscular branch
Genitofemoral nerve
Saphenous nerve
Adductor canal (of Hunter)
Abdominal Aortic Aneurysm Repair
Skin Incision (Fig. 111.1)
Technical Points
Many surgeons prefer a midline transperitoneal incision, as shown in Figures 111.1 to 111.4. Position the patient supine. Prepare and drape the abdomen from the nipples to the knees to allow a midline incision with the possibility of extending the bypass to the femoral arteries in the groin if necessary. Place a sterile towel over the genitalia and an iodophor-impregnated plastic adhesive drape over all exposed skin to protect the prosthetic graft from skin flora. Make a midline incision from the xiphoid to the midhypogastrium or symphysis pubis (Fig. 111.1A). Cover the transverse colon and omentum with a moist lap and elevate superiorly out of the abdominal cavity. Sharply mobilize the third and fourth portion of the duodenum to the right and off the infrarenal aorta by dividing the ligament of Treitz (Fig. 111.1B). Pack the small bowel in a moist towel and retract to the right. Pack and retract the descending and sigmoid colon laterally and inferiorly if necessary. The aneurysm should now be well exposed. Self-retaining retractors such as the Omni are very helpful. An alternative retroperitoneal approach is presented in Figures 111.5 and 111.6.
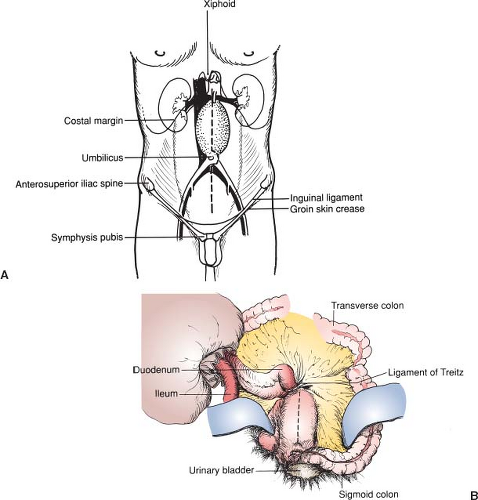 Figure 111.1 Skin incision. A: Skin incision. B: Initial exposure of aneurysm. |
Anatomic Points
The midline incision has many anatomic advantages if a transperitoneal approach is used. In addition to providing maximal exposure of the peritoneal cavity, it affords a strong closure because several fascial and aponeurotic layers fuse as the linea alba. Retraction of the transverse colon superiorly displaces the transverse mesocolon superiorly, exposing the superior aspect of the root of the mesentery, which begins at the duodenojejunal flexure. Direct visualization and palpation of the ligament of Treitz (suspensory muscle of the duodenum) is then possible. This fibromuscular band arises from the right crus of the diaphragm and then passes posterior to the pancreas and splenic veins and anterior to the left renal vasculature. It may contain numerous small vessels. Reflection of the duodenum and small bowel to the right, and of the descending and sigmoid colon to the left, exposes the aneurysm, which is covered with parietal peritoneum.
Exposure of the Infrarenal Aorta and Iliac Arteries (Fig. 111.2)
Technical Points
Open the peritoneum over the aneurysm staying slightly to the right of the midline (Fig. 111.2A). More than 90% of abdominal aortic aneurysms are infrarenal. The superior neck of the aneurysm (area of normal aorta just proximal to where the aneurysmal widening begins) then lies just distal to the renal arteries and posterior to where the renal vein crosses over the aorta. Exercise care to avoid injury to these vessels in dissecting the neck of the aneurysm for clamping. The left renal vein may be dissected circumferentially and retracted proximally with a vein retractor. Dividing the left gonadal vein, lumbar vein and adrenal vein branches will allow further retraction of the left renal vein for better visualization of the juxtarenal aorta. Rather than risk tearing the left renal vein during an unusually difficult exposure, it may be intentionally divided at the onset and oversewn adjacent to the vena cava while preserving the above branches. On reviewing films prior to surgery, look for the retroaortic left renal vein anatomic variant as it is highly susceptible to accidental injury during clamping and subsequent massive, difficult-to-control hemorrhage.
The ureters lie close to the aneurysm and are most susceptible to dissection or retraction injury where they cross anterior to the iliac bifurcation to enter the pelvis. The common iliac veins adhere closely to the arteries and should be carefully separated from them only for a distance that is sufficient to allow clamping of the arteries (Fig. 111.2B).
Aspirate blood from the inferior vena cava or aorta for preclotting of knitted Dacron grafts. Preclotting of woven, “presealed” knitted, or PTFE grafts is unnecessary. Then have the anesthesiologist administer 100-U/kg heparin intravenously. Clamp all vessels gently to avoid dislodging atheroma or thrombus
as emboli. Open the anterior wall of the aneurysm longitudinally staying to the right of the origin of the inferior mesenteric artery. Remove mural thrombus and suture-ligate bleeding lumbar arteries. At the superior and inferior necks of the aneurysm, extend the incision transversely in a T pattern through the anterior half of the wall. Leave the posterior portion intact for strong purchase of sutures. Retracting sutures or a self-retaining retractor placed in the wall of the aneurysm may be helpful. Remove any debris from both necks of the aneurysm.
as emboli. Open the anterior wall of the aneurysm longitudinally staying to the right of the origin of the inferior mesenteric artery. Remove mural thrombus and suture-ligate bleeding lumbar arteries. At the superior and inferior necks of the aneurysm, extend the incision transversely in a T pattern through the anterior half of the wall. Leave the posterior portion intact for strong purchase of sutures. Retracting sutures or a self-retaining retractor placed in the wall of the aneurysm may be helpful. Remove any debris from both necks of the aneurysm.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


