FIGURE 8-1
A. Administration of liquid medication to infants and toddlers requires gently holding the child and administering with a syringe or dropper. B. Administration of liquid medication to school-age children involves giving them choices—for example, what type of liquid to mix a medication that is distasteful. (Used with permission from Pillitteri, A. [2007]. Maternal and child health nursing [5th ed.]. Philadelphia, PA: Lippincott Williams & Wilkins, pp. 1145 and 1080.)

Dosage Based on mg/kg
The dose of most pediatric drugs is based on milligram per kilogram of body weight or body surface area (BSA) in meters squared (m2). This section shows you how to convert pounds to kilograms, how to estimate the safety of a dose, and, finally, how to determine the dose. To ensure accuracy, use a calculator. The next section will show how to determine dosage based on BSA.
Converting Ounces to Pounds
An infant weighs 20 lb 12 oz. Convert the ounces to pounds.
Step 1. Because there are 16 oz in 1 lb, divide the 12 oz by 16. You should get a decimal:

Step 2. Add the answer to the pounds to get the total number of pounds:
20 + 0.75 = 20.75 lb
EXAMPLE
An infant weighs 25 lb 6 oz. Convert the ounces to pounds.
Step 1. Divide 6 by 16:

Step 2. Add the answer to the pounds:
25 + 0.375 = 25.375 1b
Converting Pounds to Kilograms
EXAMPLE
A child weighs 33 lb. How many kilograms?
Step 1. Because there are 2.2 lb per 1 kg, divide the 33 lb by 2.2. Round off to the nearest hundredth (if necessary):

The child weighs 15 kg.
EXAMPLE
An infant weighs 18 lb 12 oz. How many kilograms?
Step 1. Convert ounces to pounds first:

Step 2. Add the answer to the pounds:
18 + 0.75 = 18.75 lb
Step 3. Convert to kilograms. Round off to the nearest hundredth:

The infant weighs 8.52 kg.
Converting Pounds to Kilograms
Convert pounds to kilograms. Use a calculator. Round the final answer to the nearest hundredths place. Answers appear at the end of the chapter.
1. 30 lb = _______________________ kg
2. 15 lb 5 oz = __________________ kg
3. 71.4 lb = _____________________ kg
4. 22 lb = _______________________ kg
5. 54 lb 8 oz = __________________ kg
6. 4 lb 5 oz = ___________________ kg
7. 75 lb = _______________________ kg
8. 12 lb 3 oz = __________________ kg
9. 66 lb = _______________________ kg
10. 101.2 lb = ___________________ kg
Steps—mg/kg Body Weight
EXAMPLE
Augmentin (amoxicillin) 150 mg po q8h is ordered for a child weighing 33 lb. Figure 8-2 shows the label for Augmentin, which comes as a dry powder. The accompanying prescribing information states that children £40 kg receive 6.7 to 13.3 mg/kg q8h.
We need to convert 33 lb to kg, calculate the low and high safe dose, determine whether the dose ordered is within the safe range, and prepare the dose. These are the steps:
STEP 1.
STEP 2.
STEP 3.
STEP 4.
Convert ounces to pounds; then convert pounds to kilograms, dividing by 2.2.
Determine the safe dose range in milligrams per kilograms by using a reference (such as a drug book or drug insert).
Decide whether the ordered dose is safe by comparing the order with the safe dose range listed in the reference.
Calculate the dose needed.

FIGURE 8-2
Label for Augmentin (amoxicillin) for oral suspension. (Courtesy of GlaxoSmithKline.)
Step 1. Convert pounds to kilograms. Divide the number of pounds by 2.2:

The child weighs 15 kg.
Step 2. Determine the safe dose range. The literature states that the dose should range from 6.7 to 13.3 mg/kg q8h.

Step 3. Is the dose safe? The safe range is 100 to 200 mg q8h. The dose ordered (150 mg q8h) is indeed safe because it falls within the 100- to 200-mg range.
Step 4. Calculate the dose.
The label states that 90 mL water should be added gradually (see Fig. 8-2) to make a concentration of 125 mg/5 mL.

Give 6 mL.
You can measure this dose with a calibrated safety dropper or oral syringe. For examples of this equipment, see Figure 8-3.

FIGURE 8-3
Examples of equipment used to obtain pediatric doses: (top) a medication spoon calculated in milliliters and teaspoons; (center) an oral syringe calculated in teaspoons; (bottom) a safety dropper calibrated in milliliters. (A regular syringe marked in milliliters may also be used.)
EXAMPLE
A child weighing 16 lb 10 oz is ordered Lasix (furosemide) 15 mg po bid (Fig. 8-4). Is the dose safe? What amount should you pour?
Step 1. Convert pounds to kilograms:
a. Change the ounces to part of a pound:
The child’s weight is 16 + 0.625 = 16.625 lb.

FIGURE 8-4
Label for Lasix (furosemide). (Used with permission of Roxane Laboratories, Inc.)
b. Change pounds to kilograms. Round off to the nearest hundredth:

The child weighs 7.56 kg.
Step 2. Determine the safe dose range in milligrams per kilogram. The package insert states: The initial dose of oral Lasix (furosemide) in infants and children is 2 mg/kg body weight, given as a single dose. If the diuretic response is not satisfactory after the initial dose, dosage may be increased by 1 or 2 mg/kg no sooner than 6 to 8 hours after the previous dose. Doses greater than 6 mg/kg body weight are not recommended.

Step 3. Decide whether the ordered dose is safe. The order is 15 mg po bid. The 15 mg meets the requirement for a single dose. The order is bid, which means twice in a day; you calculate 15 mg ´ 2 = 30 mg. The child will receive 30 mg in a day. The high range is 45 mg, so the dose is safe.
Step 4. Calculate the dose needed. The supply is 10 mg/mL (Fig. 8-4).

The label states that Lasix (furosemide) comes with a calibrated safety dropper. You can use the dropper to obtain the dose of 1.5 mL.
EXAMPLE
Lanoxin (digoxin) 37.5 mcg po ´ 1 is ordered for a premature infant weighing 1500 g. Is the dose safe? What amount should be given?
Step 1. Convert grams to kilograms (1000 grams = 1 kg):

Step 2. Determine the safe dose range in milligrams per kilogram.

The Nursing Drug Guide states that the loading dose (oral) for the premature infant is 20 to 30 mcg/kg.
Step 3. The ordered dose is 37.5 mcg.
The dose ordered is safe.
Step 4. Calculate the dose. Lanoxin (digoxin) elixir (Fig. 8-5) comes in 0.125 mg/2.5 mL or 50 mcg per milliliter.

Use a calibrated safety dropper or oral syringe (1 mL) to draw up 0.75 mL.

FIGURE 8-5
Label for Lanoxin (digoxin). (Courtesy of Roxane Laboratories, Inc.)
EXAMPLE
A child weighing 66 lb is prescribed epinephrine subcutaneous injection for an allergic reaction. The dose prescribed is 0.3 mg. Is the dose safe? What amount should be given?
Step 1. Convert pounds to kilograms:

The child weighs 30 kg.
Step 2. Determine the safe dose range in milligrams per kilogram.
The Nursing Drug Guide states 0.01 mg/kg subcutaneous every 20 minutes. Do not exceed 0.5 mg in a single dose.
Step 3. The ordered dose is 0.3 mg:

The dose is safe.
Step 4. Calculate the dose. Figure 8-6 shows a concentration of 1 mg/mL. Therefore, 0.3 mg = 0.3 mL (no calculation needed). Use a 1-mL precision syringe for the dose.

FIGURE 8-6
Label for subcutaneous and IM epinephrine. (Courtesy of American Regent, Inc.)
Dosage Calculations
In these practice problems, determine whether the doses are safe and calculate the amount needed. Round the lb to kg weight conversions to the nearest hundredth. Answers appear at the end of the chapter.
1. | Order: Child: Supply: Literature: | Amoxil (amoxicillin) 60 mg po q8h Weight 20 lb Amoxil (amoxicillin) 125 mg/5 mL 20 to 40 mg/kg/day in divided doses q8h |
2. | Order: Child: Supply: Literature: | Augmentin (amoxicillin) 175 mg po q8h Weight 29 lb Bottle of 125 mg/5 mL 40 mg/kg/day in divided doses q8h |
3. | Order: Child: Supply: Literature: | ferrous sulfate 200 mg po tid 9 years old and weighs 30 kg bottle of 125 mg/5 mL children 6 to 12 years old, 600 mg/day, in divided doses tid |
4. | Order: Child: Supply: Literature: | Tylenol (acetaminophen) 80 mg po q4° prn for temp 100.9°F and above 6 years old and weighs 20.5 kg chewable tablets 80 mg For child 6 to 8 years, give four chewable tablets. May repeat four or five times daily. Not to exceed five doses in 24 hours. |
5. | Order: Infant: Supply: Literature: | Valium (diazepam) 1 mg IM q3–4h prn 30 days old vial 5 mg/1 mL child < 6 mo IM 1 to 2.5 mg tid or qid |
6. | Order: Child: Supply: Literature: | Morphine 2 mg subcutaneous q3–4h for pain 3 years old and weighs 14 kg injection labeled 2 mg/mL starting dose 0.05 to 0.2 mg/kg; not to exceed 15 mg/dose |
7. | Order: Child: Supply: Literature: | Reglan (metoclopramide) 5 mg PO q6h 3 years old and weighs 30 kg syrup 5 mg/5 mL 0.1 to 0.2 mg/kg/dose up to four times a day. |
8. | Order: Child: Supply: Literature: | Claforan (cefotaxime) 0.5 g IM q6h Weight 48 lbs injection reconstituted 300 mg per 1 mL for children < 50 kg, 100 to 200 mg/kg/day, divided q 6 hour |
9. | Order: Child: Supply: Literature: | Zithromax (azithromycin) po 300 mg × 1 dose 10 years old and weighs 30 kg oral suspension 100 mg/5 mL in 15-mL bottle children 2 to 15 years, 10 mg/kg (not more than 500 mg/dose) on day 1 |
10. | Order: Infant: Supply: Literature: | Dilantin (phenytoin) po 60 mg bid Weight 12 lb 8 oz Dilantin (phenytoin) suspension 30 mg/5 mL 4 to 8 mg/kg/day divided into two doses. Maximum dose is 300 mg/day. |
Determining Body Surface Area in Meters Squared
A second method to determine pediatric dosage is to calculate BSA in meters squared using a chart called a nomogram (Fig. 8-7). Height is marked in the left column, weight in the right column. A line is drawn between these two marks. The point at which the line intersects the middle column indicates BSA in meters squared.
There are several mathematical formulas to calculate BSA. The following formula often is used: Average BSA for children and infants:
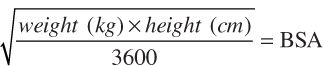
Average BSA for children and infants:
9 year olds: 1.07 m2
10 year olds: 1.14 m2
12 to 13 year olds: 1.33 m2
Neonates: 0.25 m2
2 year olds: 0.5 m2

FIGURE 8-7
Nomogram for infants and toddlers.
Because of differences in growth, charts used for infants and young children are different from those for older children and adults. If a child weighs more than 65 lb or is more than 3 feet tall, use the adult nomogram (Fig. 8-8).
EXAMPLE
1. An infant with a height of 18 inches weighing 15 lb has a BSA of 0.26 m2.
2. A child 4´2´´ weighing 130 lb has a BSA of 1.55 m2.

FIGURE 8-8
Nomogram for adults and children. To determine the surface area, draw a straight line between the point representing the patient/client’s height on the left vertical scale to the point representing the patient/client’s weight on the right vertical scale. The point at which this line intersects the middle vertical scale represents the surface area in meters squared.
BSA is used mainly in calculating chemotherapy dosages. Determining BSA can be done with a special calculator or using the Internet. One useful Web site for calculating BSA is www.globalrph.com/bsa2.htm
SELF-TEST 3
Determining Body Surface Area
Convert height and weight to BSA in meters squared using Figure 8-8 or 8-9. Answers appear at the end of this chapter.

STEP 1.
STEP 2.
STEP 3.
STEP 4.
STEPS AND RULE—m2 MEDICATION ORDERS
Find the BSA in meters squared.
Determine the safe dose range by using a reference (such as a drug book or drug insert).
Decide whether the ordered dose is safe by comparing the order with the safe dose range listed in the reference.
Calculate the dose needed.
EXAMPLE
A 2-year-old child with a weight of 27 lb 12 oz and height of 35 inches is prescribed leucovorin calcium 5.5 mg po q6h ´ 72 hours.
Literature states dose of leucovorin for rescue after methotrexate therapy is 10 mg/m2/dose q6h ´ 72 hours.
Supply: 1 mg/mL reconstituted by the pharmacy
Step 1. Use Figure 8-7.
Height, 35 inches; weight, 27 lb 12 oz (12 ounces = 0.75 or 3/4 4 lb)
Make weight 27 3/4 lbs.
BSA = 0.55 m2
Step 2. Safe dose is 10 mg/m2/dose q6h:
Step 3. Order is 5.5 mg q6h. Dose is safe.
Step 4.

Give 5.5 mL po q6h.
EXAMPLE
A 6-year-old child with a weight of 40 lb and height of 45 inches is prescribed methotrexate 7.5 mg po twice weekly.
Literature states methotrexate 7.5 to 30 mg/m2/dose twice weekly.
Supply: 2.5-mg tablets
Step 1. Use Figure 8-8.
Height, 45 inches; weight, 40 lb
BSA = 0.75
Step 2. Safe dose is 7.5 to 30 mg/m2/dose twice weekly:

Step 3. Order is 7.5 mg po twice weekly. Dose is safe.

Give 3 tablets po twice weekly.
SELF-TEST 4
Use of Nomogram
In these problems, determine whether the dose is safe, using the nomogram in Figure 8-7 or 8-8 and calculating. Answers appear at the end of the chapter.
1. | Order: Child: Supply: Literature: | Tambocor (flecainide) 50 mg po q8h 8 years; height, 50 inches; weight, 55 lb 50-mg tablets dose 100 to 200 mg/m2/24 hours in divided doses q8–12h |
2. | Order: Child: Supply: Literature: | methotrexate 12.5 mg po q week 12 years; height, 59 inches; weight, 88 lb 2.5-mg tablets 10 mg/m2/dose as needed weekly to control fever and joint inflammation in rheumatoid arthritis |
3. | Order: Infant: Supply: Literature: | Deltasone (prednisone) 5 mg po q12h 12 months; height, 30 inches; weight, 22 lb 8 oz 5 mg/5 mL syrup immunosuppressive dose 6 to 30 mg/m2/24 hours |
4. | Order: Child: Supply: Literature: | Marinol (dronabinol) po 5 mg × 1 10 years; height, 50 inches; weight, 35 kg 2.5-mg capsules dose 5 mg/m2 1 to 3 hours before chemotherapy |
5. | Order: Child: Supply: Literature: | AZT (zidovudine) po 200 mg q6h 12 years; height, 60 inches; weight, 100 lb 100-mg capsules children 3 months to 12 years, 90 to 180 mg/m2 q6h, not to exceed 200 mg q6h |

Administering IV Medications
IV medications are administered when a child cannot maintain an oral fluid intake, has fluid electrolyte imbalances, or requires IV medication. Dosages for IV medications are calculated in milligrams or micrograms per kilogram.
IV push (IVP) medications are calculated according to weight and are then administered, using the correct dilution and administration time. This information is in a drug handbook or administered per institutional policy. Continuous IV medications are also calculated according to weight and are then infused through an infusion pump.
IV piggyback (IVPB) medications are administered in small amounts of diluent. Consult a pediatric reference or institutional manual to determine the minimum and maximum safe amount of diluent. Drugs for IVPB must be initially diluted following the manufacturer’s directions. Once you make the initial dilution, withdraw from the vial the amount of drug required to obtain the dose. IVP or IVPB drugs may also be administered with a syringe pump, which will safely deliver the medication over a specific period of time (Fig. 8-9).
Buretrols, volutrols, or other volume control units are used to administer IV fluids (Fig. 8-10). Buretrols are calibrated; they hold only 100 to 150 mL at a time, thus reducing the possibility of fluid overload. Buretrols are attached to the primary IV fluid bag. In the pediatric setting, Buretrols are usually filled with only 1 to 2 hours worth of IV fluid, so the nurse is responsible for checking the IV frequently to make sure the IV site has not infiltrated or to make sure the child is not receiving too much or too little fluid or medication. Drugs for IVPB that have been diluted can be added to a Buretrol (Fig. 8-11).
For smaller children and infants requiring IVPB medications, the medication is usually added to only 10 to 50 mL in the Buretrol, although this amount varies depending on the size and age of the child, fluid restrictions, and other factors. Always follow institutional policy regarding IV infusions.
When the Buretrol is empty of the IV medication, much of the drug will still be in the tubing. For this reason, you need to add an IV flush of 15 to 30 mL to the Buretrol after the medication is infused to ensure that the child receives the drug. This amount varies according to the length of tubing and any extension IV tubing. Follow institutional policy regarding the amount. For this text, we will use 20 mL of IV flush in the Buretrol, after the medication has infused.
Infusion pumps provide a second safeguard (Fig. 8-12). To ensure that pediatric patients/clients receive accurate dosing, you can set infusion pump rates in tenths and hundredths. In neonatal areas, syringe pumps can deliver IV fluid ranging from 1 to 60 mL. Many hospitals use premixed IVPB solutions (from the hospital pharmacy) or syringe pumps are used in place of IVPB (Fig. 8-9). The syringe pump has the medication in a large syringe, attached to a special pump, that can then deliver the medication in a specific amount of time.

FIGURE 8-9
Syringe Pump. (Courtesy of Hospira, Inc.)

FIGURE 8-10
Volume control infusion device (Buretrol). (Used with permission from Taylor, C. [2008]. Fundamentals of nursing [6th ed.]. Philadelphia, PA: Lippincott Williams & Wilkins, p. 853.)

FIGURE 8-11
Adding medication to a volume control infusion device (Buretrol). (Used with permission from Taylor, C. [2008]. Fundamentals of nursing [6th ed.]. Philadelphia, PA: Lippincott Williams & Wilkins, p. 854.)

FIGURE 8-12
An infusion pump with a volume control device. (With permission from Pillitteri, A. [2002]. Maternal and child health nursing [4th ed.]. Philadelphia, PA: Lippincott Williams & Wilkins, p. 1106.)
This section considers the calculation of pediatric doses for IVP and IVPB administration.
STEP 1.
STEP 2.
STEP 3.
STEP 4.
STEP 5.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


