INTRODUCTION
Modern surgery has been redefined by powered instruments, technological tools that in many ways have revolutionized the delicacy, precision, and accuracy of the various operations performed. Yet many people who use these implements every day have very little understanding of the technology behind these tools. Although a complete treatise on electromagnetic generation of heat and the physics of current generation are beyond the scope of this chapter (and are available elsewhere), understanding some fundamental rules governing the behavior of electrical currents and some relatively straightforward principles helps guide the use of these technologies.
ELECTROSURGERY
An electrical circuit is any pathway that allows the uninterrupted flow of electrons. Electrical current is the flow of electricity (the number of electrons) in a given circuit over a constant period of time and is measured in amperes (A). Current can be supplied either as direct current (DC) with constant positive and negative terminals or as alternating current (AC) with constantly reversing poles. The electromotive force, or voltage, is a measurement of the force that propels the current of electrons and is related to the difference in potential energy between two terminals. The resistance is the tendency of any component of a circuit to resist the flow of electrons and applies to DC circuits. The equivalent of this tendency in an AC circuit is known as impedance. Any electromagnetic wave, from household electricity to radio broadcasts to visible light, can be described by three components: speed, frequency, and wavelength. Because all electromagnetic waves travel at the speed of light, which is a constant, these waves depend on the relationship between their frequency and wavelength. Since these three characteristics are defined by the equation:
frequency (f) and wavelength (λ) are inversely related; that is, as frequency increases, wavelength decreases, and vice versa. The ability to pass high-frequency current through the human body without causing excess damage makes electrosurgery possible.
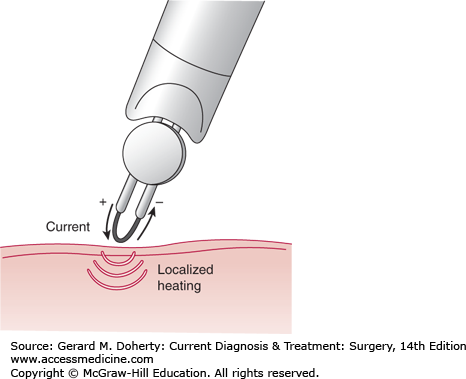
Electrosurgery is often incorrectly termed electrocautery, which is a separate technique. Electrocautery is a closed-circuit DC device in which current is passed through an exposed wire offering resistance to the current (Figure 7–1). The resistance causes some of the electrical energy to be dissipated as heat, increasing the temperature of the wire, which then heats tissue. In true electrocautery, no current passes through the patient. Electrocautery is primarily applied for microsurgery, such as ophthalmologic procedures, where a very small amount of heat will produce the desired effect or where more heat or current may be dangerous.
True electrosurgery, colloquially referred to as the “Bovie” (following its inventor, William T. Bovie, engineer and collaborator of Harvey Cushing), is perhaps the most ubiquitous power source in surgery. While the principle of using heat to cauterize bleeding wounds dates back to the third millennium bc, the directed use of electrical current to produce these effects is a far more recent development. While other scientists and engineers made significant contributions to the development of this new technology, it was Bovie who refined the electrical generator and made it practical and applicable to everyday surgery. At the most fundamental level, electrosurgery uses high-frequency (radiofrequency) electromagnetic waves to produce a localized heating of tissues, leading to localized tissue destruction. The effect produced (cutting vs coagulation) depends on how this energy is supplied.
A useful exercise to understand the way electrosurgery works is to follow the flow of current from the power outlet as it travels through the patient and returns to the wall outlet. By convention, charge is depicted as moving from positive (cathode) to negative (anode) despite that the particles that are actually moving are electrons, which have a negative charge. These descriptions are based on that convention, following the flow of positive charge.
The electrosurgical circuit consists of four primary parts: the electrosurgical generator, the active electrode, the patient, and the return electrode. Current flows from the electrosurgical generator after it is modulated to a high-frequency, short wavelength current and where multiple waveforms can be produced. (The importance of the waveform is discussed in later sections.) The current flows from the machine, through the handpiece, out the tip of the device, to the patient. If the patient were not connected in some way either to a negative terminal or to ground, no current would flow, as there would be no way to complete the circuit, hence nowhere for the charge to go. However, the patient is always connected to the electrosurgical generator by a return electrode, which allows the charge delivered by the electrosurgical probe to pass through the patient, exerting its effect, and back to the generator, completing the circuit. In reality, the term monopolar circuit is incorrect, as there are in fact two poles (the active and return electrodes); it is distinguished from bipolar electrosurgery in which both electrodes are under the surgeon’s direct control (Figure 7–2A).
Figure 7–2.
A. In monopolar electrosurgery, current from an electrosurgical generator passes from an active electrode (the “Bovie” tip) through the patient to a return electrode of greater area. B. In bipolar electrosurgery, the active and return electrodes are in the handpiece, and current only flows through the surgical site.
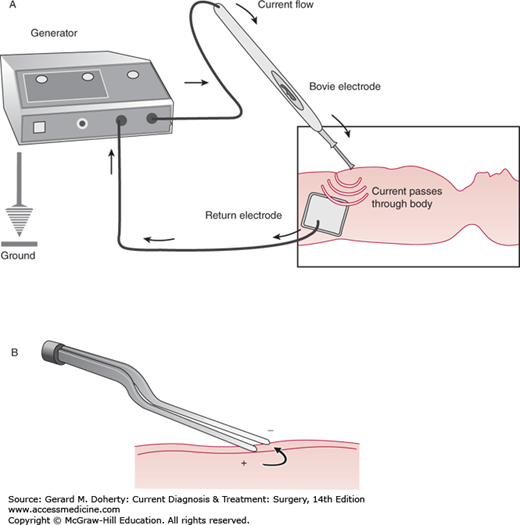
The essential components of the bipolar electrosurgical circuit are the same as those in the monopolar circuit; however, in this system, the active and return electrodes are in the same surgical instrument. In this technique, high-frequency current is passed through the active electrode and through the patient to heat and disrupt tissue. In this arrangement, however, the return electrode is in the handpiece, as the opposite pole of the active electrode. This method enables the surgeon to heat only a discrete amount of tissue (Figure 7–2B).
The current that powers the electrosurgical generator is supplied at a frequency of 60 Hz. This type of electromagnetic energy can indeed cause very strong (potentially lethal) neuromuscular stimulation, making it unsuitable for use in its pure form. Muscle and nerve stimulation, however, ceases at around 100 kHz. Current with a frequency above this threshold can be delivered safely, without the risk of electrocution. The outputs of electrosurgical generators deliver current with a frequency greater than 200 kHz. Current at this frequency is known as radiofrequency (RF); it is in the same portion of the spectrum as some radio transmitters. This level of RF, released from a radio antenna, can produce serious RF burns if the proper precautions are not taken.
Applying electrosurgical current to a patient produces localized tissue destruction via intense heat production, yet barring a mishap, no other lesions are produced during application of this technique. The reason the effect is exerted only at the site where the surgeon is operating, and not at the site of the return electrode, is that the surface area by which the charge is delivered is much smaller than that to which it returns. Thus, there is a far greater density of charge at the site of the handpiece (“active” electrode) contact than there is at the site of return. If there is another connection between the patient and ground that offers less resistance to the flow of current, and if it also comprises a relatively small surface area, then the patient could be in danger of suffering an electrosurgical burn. Similarly, it is possible that if the return electrode were to be damaged, or if contact was not maintained, a burn could occur in this area. The possibility of a burn at the site of the return electrode is eliminated in most modern machines by the presence of a monitoring system that assesses the completeness of contact (by maintaining a smaller, secondary circuit) and automatically disables power if full contact of the pad is lost (as could be caused by tripping over a wire and tearing the return pad).
All types of electrosurgery exert their effects via the localized production of heat and the subsequent changes in the heated tissue. Therefore, the different effects produced by electrosurgical instruments are created by altering the manner in which this heat is produced and delivered. Adjustment is made possible by altering the wave pattern of the current.
Cutting depends on the production of a continuous sine wave of current (Figure 7–3A
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


