CHAPTER 62 Posterior abdominal wall and retroperitoneum
The posterior abdominal wall consists of fasciae, muscles and their vessels and spinal nerves; the overlying skin is continuous with that of the back. It is not easily defined, and is best described as that part of the abdominal wall lying between the two mid-dorsal lines, below the posterior attachments of the diaphragm and above the pelvis. It is continuous laterally with the anterolateral abdominal wall, superiorly with the posterior wall of the thorax behind the attachments of the diaphragm and inferiorly with the structures of the pelvis. The spinal column forms part of its structure and the muscles and fasciae of the back are closely related to it, especially posterolaterally.
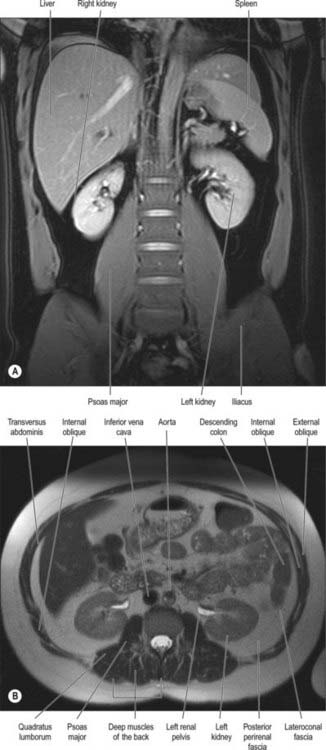
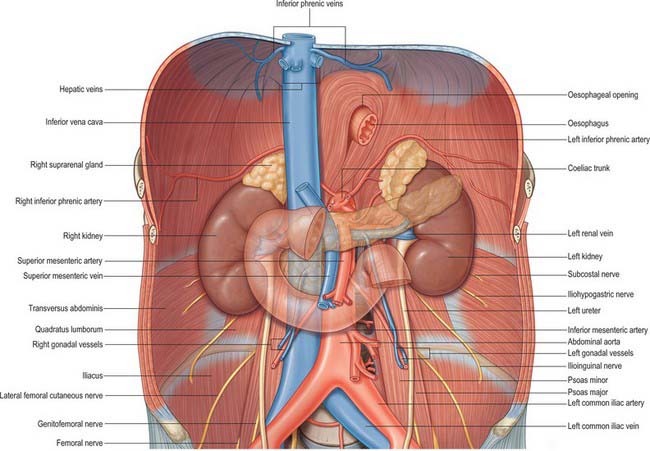
The major vessels and lymphatic channels, in addition to the peripheral autonomic nervous systems of the abdomen, pelvis and lower limbs lie on the posterior abdominal wall. These structures, together with several viscera (including the kidneys [Ch. 74], suprarenal glands [Ch. 72], pancreas [Ch. 70], ureters [Ch. 74] and parts of the gut tube [Chs 66 and 67]), lie beneath the posterior parietal peritoneum. These tissues and their surrounding connective and fascial planes are collectively referred to as the retroperitoneum.
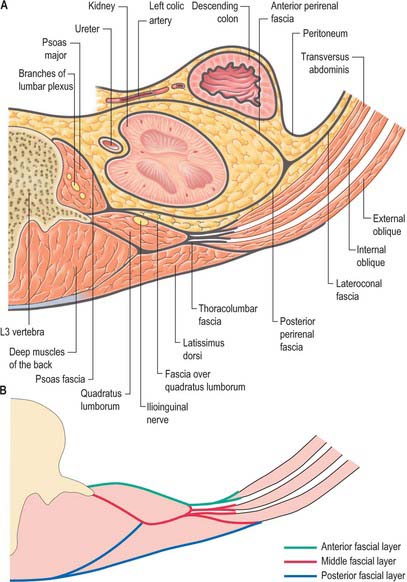
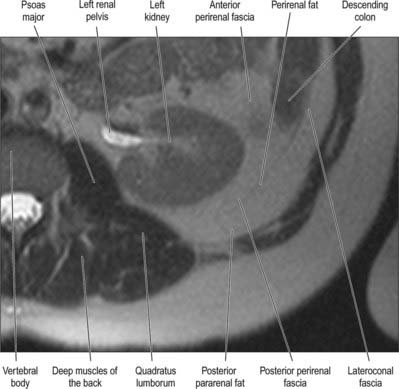
It has been suggested that the retroperitoneum can be divided into several spaces according to their relationships to the fascial layers that surround the kidneys and ureters. In this description, the layers of the perirenal fascia enclose a perirenal space containing the kidney, suprarenal gland, upper ureter and their neurovascular supply. The anterior layer of the perirenal fascia is continuous across the midline anterior to the main neurovascular structures of the retroperitoneum, and the right and left perirenal spaces communicate, although this channel is limited and contains many of the midline neurovascular structures of the retroperitoneum. Behind the posterior layer of the perirenal fascia lies the posterior pararenal space. Anterior to the anterior layer of the perirenal fascia lies the anterior pararenal space, in which lie several retroperitoneal parts of the gut tube, including the duodenum and pancreas. The anterior pararenal spaces are also continuous across the midline and are limited posteriorly by the anterior communicating layer of the perirenal fascia and anteriorly by the parietal peritoneum. This description helps to explain why moderate amounts of fluid, blood or pus collecting in the retroperitoneum tend to remain constrained within the space in which they are formed although, for pathological processes such as tumour invasion, the fascial planes provide a weak barrier to local spread (Figs 62.1, 62.2).
SKIN AND SOFT TISSUES
THORACOLUMBAR FASCIA
The thoracolumbar fascia in the lumbar region is in three layers (Figs 62.1, 62.2, 62.3). The posterior layer is attached to the spines of the lumbar and sacral vertebrae and to the supraspinous ligaments. The middle layer is attached medially to the tips of the transverse processes of the lumbar vertebrae and the intertransverse ligaments, inferiorly to the iliac crest, and superiorly to the lower border of the 12th rib and the lumbocostal ligament. The anterior layer covers quadratus lumborum and is attached medially to the anterior surfaces of the transverse processes of the lumbar vertebrae behind the lateral part of psoas major. Inferiorly, it is attached to the iliolumbar ligament and the adjoining part of the iliac crest. Superiorly, it is attached to the apex and inferior border of the 12th rib and then extends to the transverse process of the first lumbar vertebra, to form the lateral arcuate ligament of the diaphragm. The posterior and middle layers of the thoracolumbar fascia unite at the lateral margin of erector spinae. At the lateral border of quadratus lumborum they are joined by the anterior layer, to form the aponeurotic origin of transversus abdominis.
OTHER FASCIAL LAYERS
Perirenal fascia
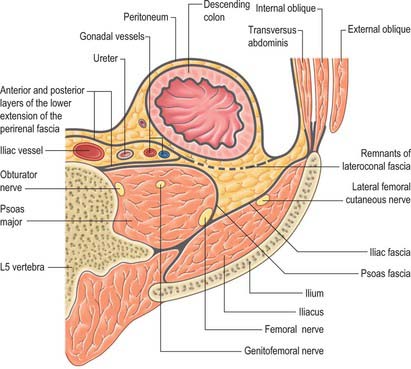
The perirenal fascia is a multilaminated fascial layer that surrounds the kidney, suprarenal glands, upper ureter and associated fat, which all lie in the perirenal space (see Ch. 74). Although described as having anterior and posterior layers, these are continuous with each other laterally, and give rise to the lateroconal fascia at this point (Figs 62.1–62.3). The posterior layer of the renal fascia is adherent to the fascia over psoas major, the iliac fascia and the anterior layers of the thoracolumbar fascia. In the obese, there may be some loose adipose tissue between these layers, but it is rarely thick. The anterior part of the renal fascia separates the kidney and the perirenal space from the overlying anterior pararenal space and its associated viscera (on the right the duodenum, ascending colon and right colonic mesentery and on the left the duodenum, descending colon and left colonic mesentery). Inferiorly, the perirenal fascia continues down and encloses the ureter. It becomes progressively thinner towards the brim of the pelvis, where it is no longer distinguishable from the loose general connective tissue of the retroperitoneum.
MUSCLES
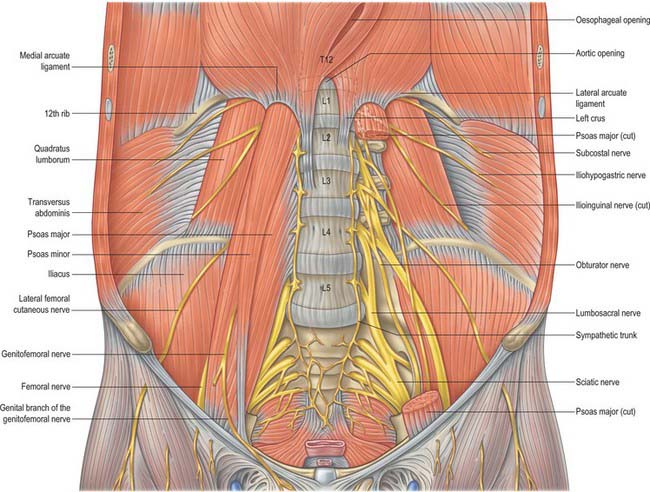
The majority of the muscles of the posterior abdominal wall are functionally part of the lower limb or vertebral column. They provide the surface against which the neurovascular structures of the retroperitoneum lie, and they are supported and separated from the majority of the retroperitoneal structures by fascial layers (Figs 62.4, 62.5; see Fig. 62.14).
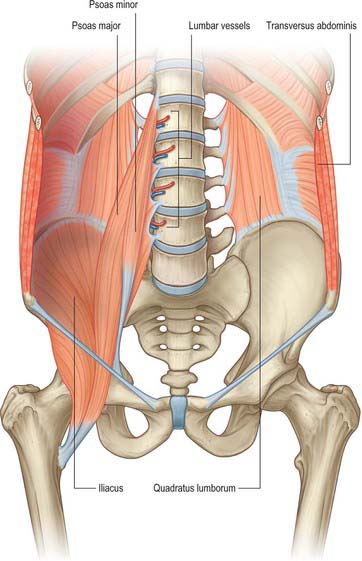
Quadratus lumborum
Quadratus lumborum is attached below by aponeurotic fibres to the iliolumbar ligament and the adjacent portion of the iliac crest for approximately 5 cm. The superior attachment is to the medial half of the lower border of the 12th rib, and by four small tendons to the apices of the transverse processes of the upper four lumbar vertebrae. Sometimes it is also attached to the transverse process or body of the 12th thoracic vertebra. Occasionally, a second layer of this muscle is found in front of the first, attached to the upper borders of the transverse processes of the lower three or four lumbar vertebrae and to the lower margin and the lower part of the anterior surface of the 12th rib.
Erector spinae
The muscles of the erector spinae group (see Ch. 42) do not form part of the posterior abdominal wall itself, but are closely associated with the fascial layers of the posterior wall.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
ABDOMINAL AORTA
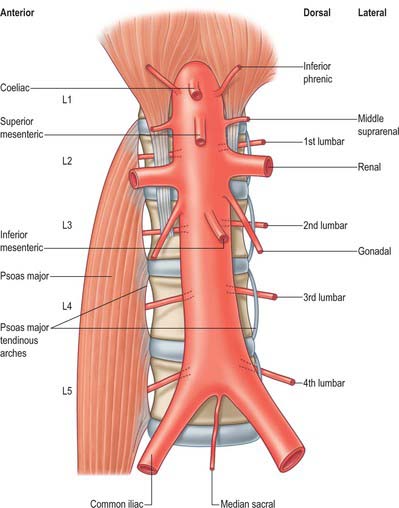
The abdominal aorta begins at the median, aortic hiatus of the diaphragm, anterior to the inferior border of the 12th thoracic vertebra and the thoracolumbar intervertebral disc (Figs 62.6, 62.7). It descends anterior to the lumbar vertebrae to end at the lower border of the fourth lumbar vertebra, a little to the left of the midline, by dividing into two common iliac arteries. It diminishes rapidly in calibre from above downward, because its branches are large; however, the diameter of the vessel at any given height tends to increase slightly with age. The cadaveric superior and inferior calibres are between 9–14 mm and 8–12 mm, respectively, with little difference between the sexes. The angle of the aortic bifurcation varies widely, particularly in the elderly. It has been suggested that the relationship between aortic size and shape is a possible causative factor in the development of abdominal aortic aneurysm (Newman et al 1971). The reflection of transmitted pressure waves at junctions between vessels (of which the abdominal aorta has many) may focally weaken the intimal lining, e.g. at the aortic bifurcation, pressure oscillations and possibly turbulence may be set up as a result of differences in the luminal diameters of the common iliac arteries, producing reflected waves that may injure the intima of the distal abdominal aorta. The role of the relative calibres of the iliac arteries remains uncertain (Shah et al 1978).
Relations
The thoracolumbar intervertebral discs, the upper four lumbar vertebrae, intervening intervertebral discs and the anterior longitudinal ligament are all posterior to the abdominal aorta. Lumbar arteries arise from its dorsal aspect and cross posterior to it. The third and fourth (and sometimes second) left lumbar veins also cross behind it to reach the inferior vena cava. The aorta may overlap the anterior border of the left psoas major.
Branches
The branches of the aorta are described as anterior, lateral and dorsal (Fig. 62.8). The anterior and lateral branches are distributed to the viscera and the dorsal branches supply the body wall, vertebral column, vertebral canal and its contents. The aorta terminates by dividing into the right and left common iliac arteries.