Pneumocystosis
Key Facts
Terminology
Lung infection caused by fungus Pneumocystis jiroveci (formerly P. carinii)
Clinical Issues
Infantile form (“plasma cell interstitial pneumonia”) affects premature and malnourished infants
Adult (sporadic) form occurs in AIDS patients and other immunocompromised patients with impaired CD4(+) lymphoid cells
Insidious onset with respiratory and generalized symptoms of fever, dyspnea, tachypnea, cough, weight loss, and fatigue
Favorable prognosis when appropriately treated; relapses are common in AIDS patients
Microscopic Pathology
Typical pattern is characterized by foamy, granular eosinophilic intraalveolar exudates containing organisms
Alveolar exudate is composed of fibrin admixed with abundant trophozoites and cysts, surfactant, and cellular debris
Cysts are oval (4-7 µm) with collapsed or crescentic forms and exhibit grooves, folds, and dark-staining central dots
Ancillary Tests
Cysts are best stained in tissues with GMS
Antibodies against Pneumocystis can be used to highlight organisms in tissue sections by immunoperoxidase technique
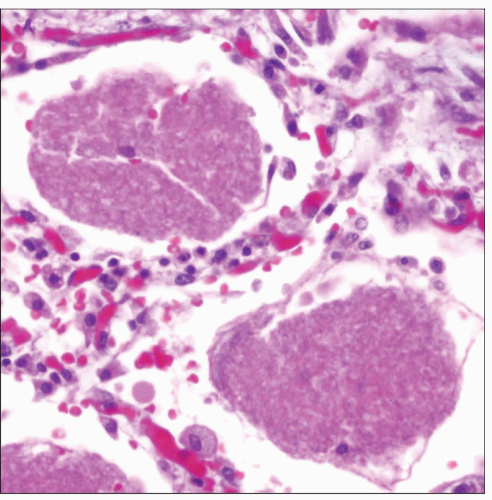 Histologic appearance of pulmonary pneumocystosis is characterized by abundant frothy intraalveolar eosinophilic exudates that contain multiple organisms. |
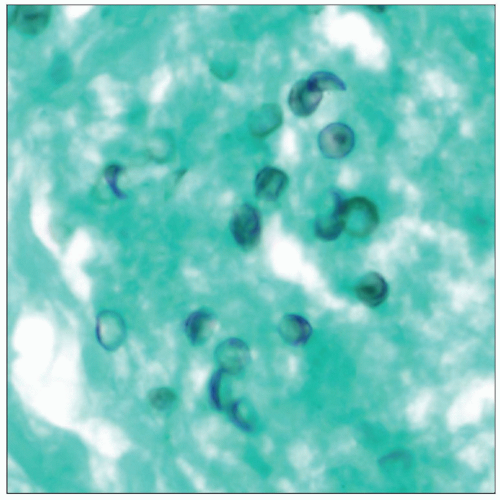 Histochemical stain for GMS in pulmonary pneumocystosis shows the typical organisms with crescentic forms as well as some cysts with dark-staining central dots. |
TERMINOLOGY
Abbreviations
Pneumocystosis pneumonia (PCP)
Definitions
Lung infection caused by fungus Pneumocystis jiroveci (formerly P. carinii)
CLINICAL ISSUES
Epidemiology
Incidence
Organisms are globally distributed
Presentation
Clinical presentation of Pneumocystis pneumonia can be quite variable
Some patients may be completely asymptomatic or show only minimal symptoms, including
Nonproductive cough, dyspnea, fever
Some patients may follow a rapidly fatal course with progressive respiratory failure
Laboratory Tests
HIV-infected patients with CD4 counts < 200 cell/µL are 5x more likely to develop PCP
Natural History
Infection is acquired by inhalation, with primary infection occurring early in life and remaining latent in host
Reinfection occurs when host becomes immunocompromised
2 major clinical forms
Infantile form (“plasma cell interstitial pneumonia”) affects premature and malnourished infants
Adult (sporadic) form occurs in AIDS patients and other immunocompromised patients with impaired CD4(+) lymphoid cells
Insidious onset with respiratory and generalized symptoms of fever, dyspnea, tachypnea, cough, weight loss, and fatigue
Favorable prognosis when appropriately treated; relapses are common in AIDS patients
Treatment
Drugs
Trimethoprim-sulfamethoxazole
Pentamidine isethionate
Early adjunctive treatment with corticosteroids can reduce morbidity and mortality
Prognosis
Survival rates of 50-90% with appropriate treatment
IMAGE FINDINGS
Radiographic Findings
Early stages show a fine pattern of ground-glass opacities involving perihilar regions
Untreated cases progress to perihilar or diffuse bilateral airspace consolidation involving mainly lower lobes
CT Findings
HRCT shows characteristic symmetrical, bilateral ground-glass opacities with geographic distribution
AIDS patients show tendency to develop bilateral thin-walled cysts in 30% of cases showing subpleural distribution
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


