TABLE 12.1 Most Common Tumors and Tumorlike Lesions of the Pituitary Gland and Sellar Region | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
and export. Identification of normal and neoplastic pituitary cell types requires attention to such features as cell shape; the content and disposition of organelles; the presence or absence and arrangement of filaments; and of course, the number, size, electron density, and shape of secretory granules (Table 12.4). The mechanisms of hormone secretion vary from transmembrane diffusion to the actual expulsion of secretory granules, a characteristic of PRL cells (7).
TABLE 12.2 Normal Anterior Pituitary Gland: Cellular and Hormonal Features | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
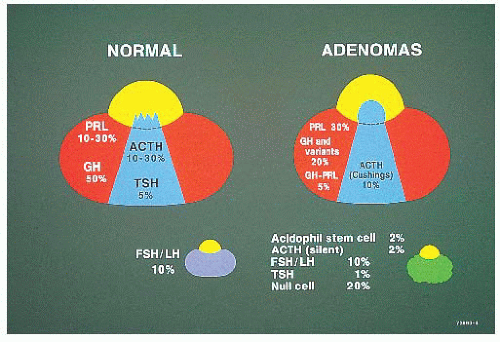 FIGURE 12.1 Schematic of the normal pituitary in horizontal section. Note the proportions and distribution of normal cells and of adenomas. To a significant extent, the locations of growth hormone (GH), prolactin (PRL), and adrenocorticotropic hormone (ACTH) adenomas correspond to the locations of their normal cellular counterparts. Clinically “silent” tumors without endocrine function are usually macroadenomas without specific localization (lower right). |
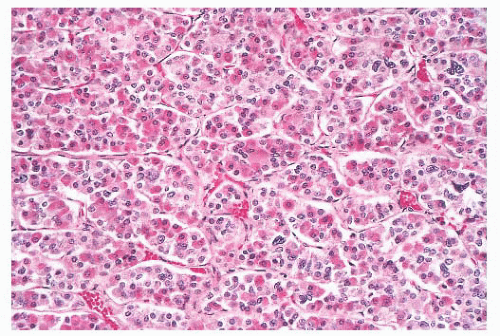 FIGURE 12.2 Normal anterior pituitary. Note the variation in cellular granularity. The staining ranges from acidophilic to chromophobic; several dark-staining basophils are also present. |
TABLE 12.3 Pituitary Adenomas: Clinical and Pathologic Characteristics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 12.4 Pituitary Adenomas: Ultrastructural Features | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
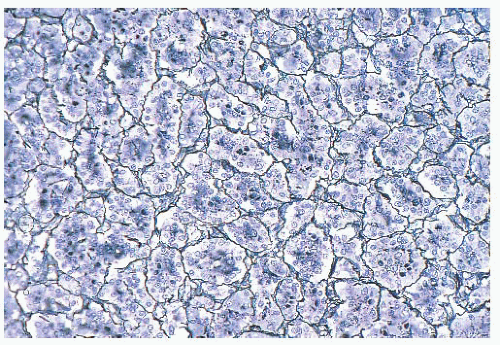 FIGURE 12.3 Normal anterior pituitary. Acini and cords of cells are demonstrated (reticulin stain). |
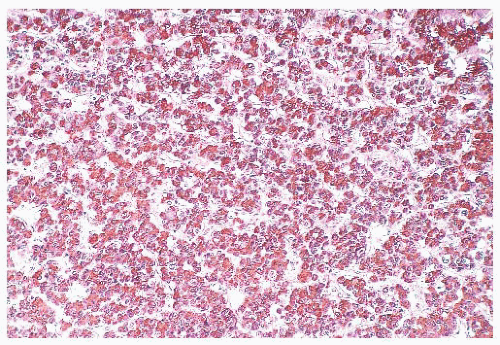 FIGURE 12.4 Normal growth hormone (GH) cells. The high density of these cells in the lateral wing of the anterior lobe, which here are seen immunostained for GH, is sufficient to mimic adenomas, particularly on frozen section. |
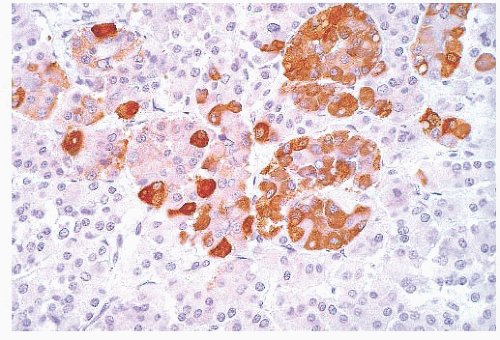 FIGURE 12.5 Normal adrenocorticotropic hormone (ACTH) cells. The nodularity normally exhibited by some ACTH cells may be mistaken for pituitary hyperplasia, particularly in the setting of Cushing disease when no adenoma is identified. |
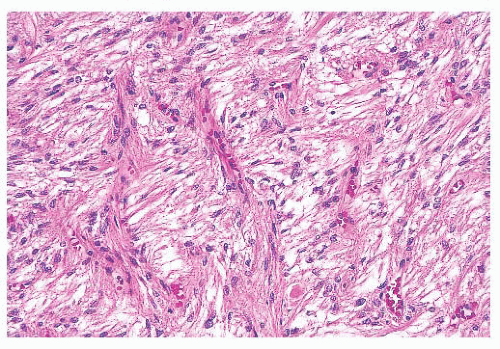 FIGURE 12.6 Posterior pituitary. The posterior lobe consists of the axonal processes and terminations of the vasopressin and oxytocin-producing supraoptic and paraventricular nuclei. In addition, endothelial cells and pituicytes, modified astrocytes, contribute to its cellularity. |
(ACTH-secreting cells). Their accumulation with age, a process termed basophil invasion of the posterior lobe, is of unknown clinical significance. Such cells are believed by some to give rise to so-called silent corticotroph cell adenomas (5,11).
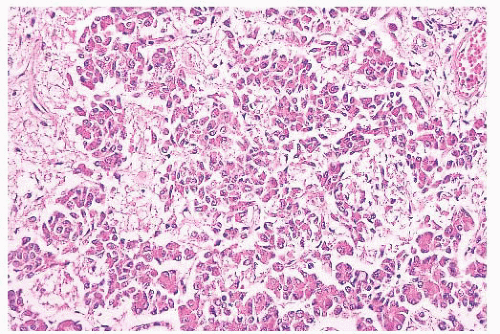 FIGURE 12.7 Basophil invasion. A normal feature of the posterior lobe is the presence of adrenocorticotropic hormone cells at its interface with the anterior lobe (periodic acid-Schiff). |
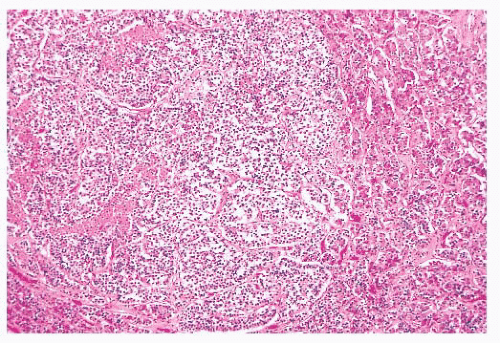 FIGURE 12.8 Microadenoma. Relative circumscription and early compression of surrounding parenchyma are seen. The acinar architecture is effaced. |
prone. The specimens usually consist of blood and necrotic tumor. Identification of the underlying tumor is aided by reticulin stains, which highlight the abnormal stromal pattern of the adenoma (Fig. 12.11).
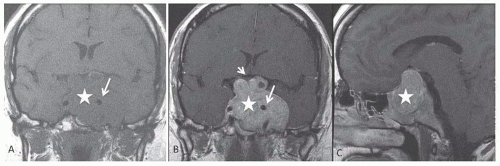 FIGURE 12.9 Macroadenoma. Coronal pre- and postcontrast T1 (A,B) and sagittal postcontrast T1 (C)-weighted sequences demonstrate a large sellar mass lesion (white star), which expands the sella and completely replaces the normal pituitary gland. The infundibular stalk is not identified. The lesion has significant suprasellar extension with left cavernous sinus invasion with encasement of the left internal carotid artery (long white arrow in A and B). Note the mass effect on the optic chiasma (short white arrow in B), which is stretched and thinned over the superior aspect of the lesion. (Courtesy of Dr. Sugoto Mukherjee, Department of Radiology, University of Virginia Health System, Charlottesville, VA). |
 FIGURE 12.10 Pituitary apoplexy. The sellar region in coronal sections shows a massive hemorrhage within a macroadenoma. (Courtesy of Dr. K. Kovacs, St. Michael’s Hospital, Toronto, Ontario, Canada.) |
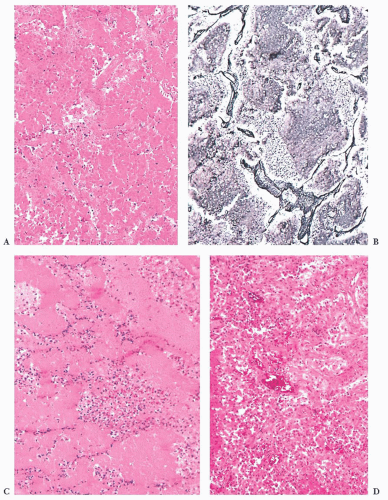 FIGURE 12.11 Pituitary apoplexy. (A) Hematoxylin and eosin-stained sections of such specimens often show only hemorrhage and extensive necrosis. (B) The underlying pattern of adenoma is highlighted by reticulin stain. (C) In the subacute phase, aggregates of polymorphonuclear leukocytes should not be mistaken for infection. (D) In chronic phases, ingrowth of granulation tissue may be conspicuous. |
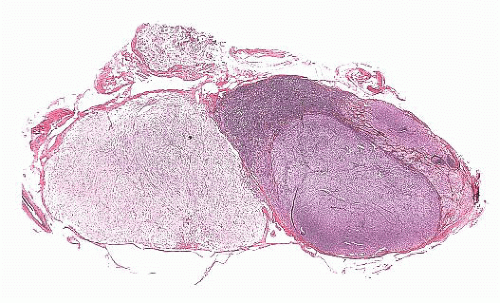 FIGURE 12.12 Microinvasive adenoma. This whole-mount sagittal section of the pituitary demonstrates the adenoma. Note the irregular outlines of the tumor, as well as the early invasion of the dural capsule, on the anterior aspect of the gland. |
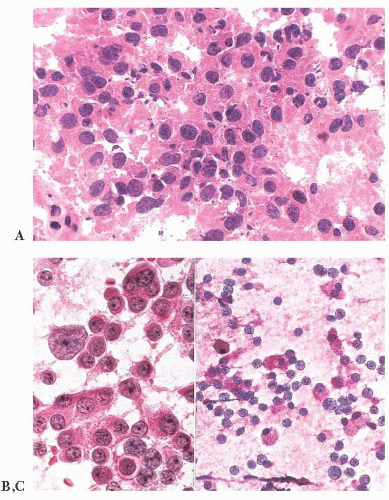 FIGURE 12.13 Pituitary adenoma. This is a comparison of a hematoxylin and eosin-stained frozen section (A) and a touch preparation (B). The latter shows excellent cytologic detail, including prominence of nucleoli, binucleation, nuclear atypia, the presence of a mitosis, and cytoplasmic uniformity. A touch preparation from normal pituitary tissue is far less cellular; it shows variation in cytoplasmic staining; and it lacks both nuclear abnormalities, as well as mitoses (C). |
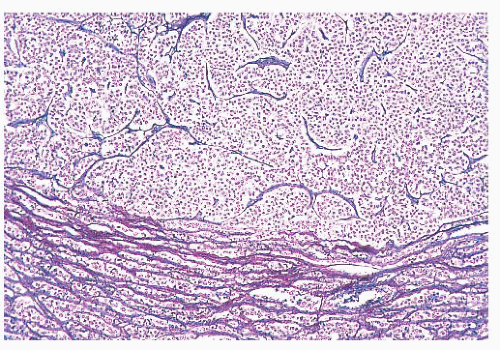 FIGURE 12.14 Pituitary adenoma. The lack of reticulin content and the compression of surrounding parenchyma are demonstrated (reticulin stain). |
cells. Although the majority of prolactinomas are medically treated by dopamine agonists, a significant number of the patients undergo surgical resection due to several clinical issues (17,18).
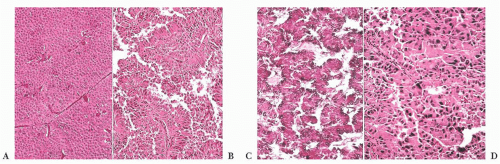 FIGURE 12.15 Pituitary adenomas. The hematoxylin and eosin-stained appearance of these adenomas, which include diffuse (A), papillary (B), ribbon (C), and pleomorphic (D) patterns, illustrates their broad morphologic spectrum and highlights the diagnostic use of immunohistochemistry. |
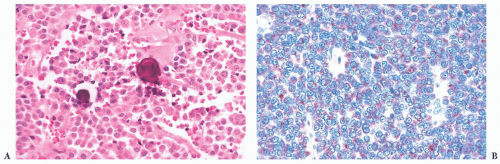 FIGURE 12.16 Prolactin cell adenomas. These are nearly all chromophobic, and they often contain spherical microcalcifications (A). Immunoreactivity for prolactin shows a characteristic globular reaction in the paranuclear Golgi zone (B). |
does the rare finding of spherical amyloid bodies (Fig. 12.17) (50). Immunoreactivity for PRL is typically strong but is paranuclear in location (Fig. 12.16). The ultrastructural features of PRL cell adenoma are distinctive (Table 12.4) and include abundant rough endoplasmic reticulum, as well as “misplaced exocytosis” or granule extrusion between neoplastic cells (37,38).
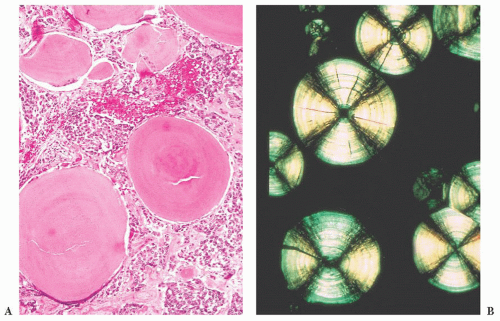 FIGURE 12.17 Prolactinoma with amyloid deposition. Such spherical bodies are virtually diagnostic of a prolactin cell adenoma (B, polarization). |
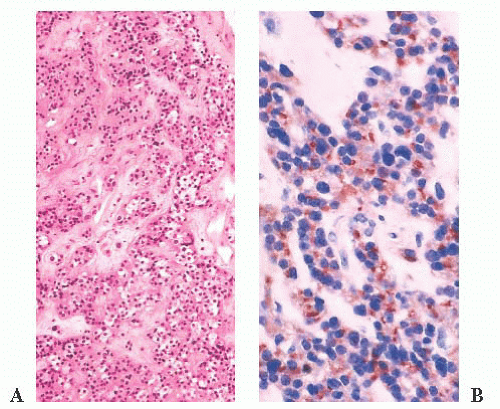 FIGURE 12.18 Treated prolactin (PRL) cell adenoma. Microscopically, these adenomas show perivascular fibrosis, which here is seen on hematoxylin and eosin stain (A) and on immunostain for PRL (B), the reactivity of which persists. |
(IGF-1) produced by the liver and more reliably elevated than GH levels.
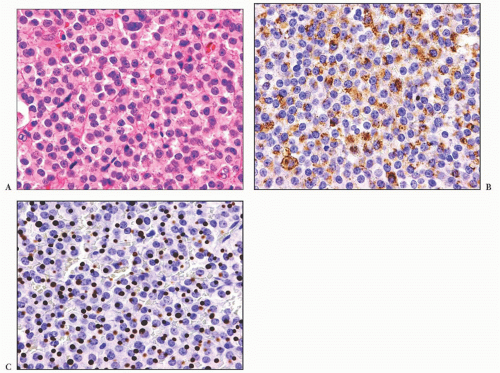 FIGURE 12.19 (A) Growth hormone cell adenoma, sparsely granulated (chromophobic) type. Note the presence of paranuclear hyaline, fibrous bodies. (B) Immunoreactivity for growth hormone may be weak and present in only a portion of cells. (C) Immunoreactivity for cytokeratin (CAM 5.2) highlights the fibrous bodies. |
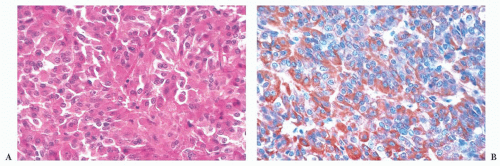 FIGURE 12.20 (A) Growth hormone (GH) cell adenoma, densely granulated (eosinophilic) type. Note the prominent acidophilia and the lack of fibrous bodies. (B) GH immunoreactivity is strong. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


