in general surgical pathology are also employed. Specific uses of histochemical stains and immunohistochemistry will be discussed along with the diseases in which their use is of value (1,2,3 and 4).
TABLE 1.1 Definitions of Dermatopathology Terms | ||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 1.2 A Few Important Clinical Terms | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
denominator of spongiotic dermatitis is the presence of intraepidermal edema, which is referred to as spongiosis because the clear spaces separating the keratinocytes impart a spongy appearance to the epidermis. Spongiotic dermatitis is subclassified into acute, subacute, and chronic subtypes, depending on the presence or absence of several additional features that are discussed later. These terms relate loosely to the chronologic evolution of the spongiotic lesion. In summary, spongiotic dermatitis comprises a spectrum of histopathologic changes, with the acute and chronic subtypes at the polar ends and the subacute subtype occupying the broad middle.
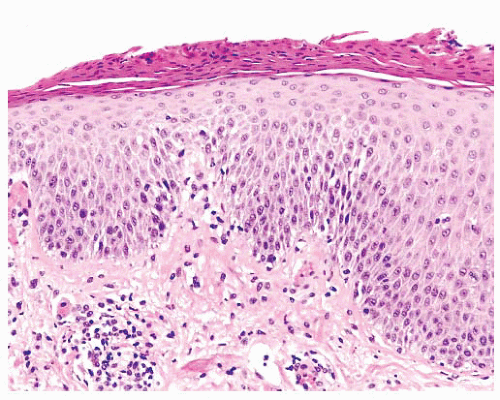 FIGURE 1.1 Subacute spongiotic dermatitis. Epidermal parakeratosis, acanthosis, intraepidermal intercellular edema (spongiosis), and lymphocytic exocytosis. A perivascular lymphocytic inflammatory infiltrate with occasional eosinophils is present in the superficial dermis. |
 FIGURE 1.2 Lichen simplex chronicus. Orthokeratosis and hypergranulosis with marked irregular acanthosis with minimal spongiosis. The underlying dermis is fibrotic. |
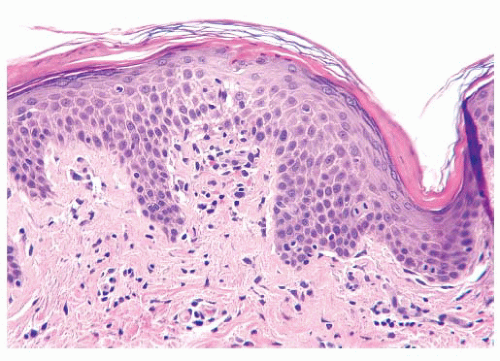 FIGURE 1.3 Pityriasis rosea. Focally mounded epidermal parakeratosis, mild spongiosis, and a perivascular lymphocytic inflammatory infiltrate in the papillary dermis. |
from the dermal infiltrate in conjunction with the described epidermal changes aids in separating pityriasis rosea from secondary syphilis, although plasma cells are not always present in the dermal infiltrate of secondary syphilis. Treponemal immunohistochemistry is useful to exclude syphilis. In addition, correlation with treponemal serologic studies is advised if there is clinical suspicion for secondary syphilis.
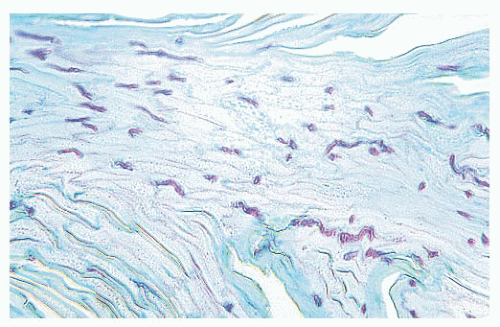 FIGURE 1.4 Dermatophytosis. Numerous fungal hyphae are present in the stratum corneum in a section stained with periodic acid-Schiff. |
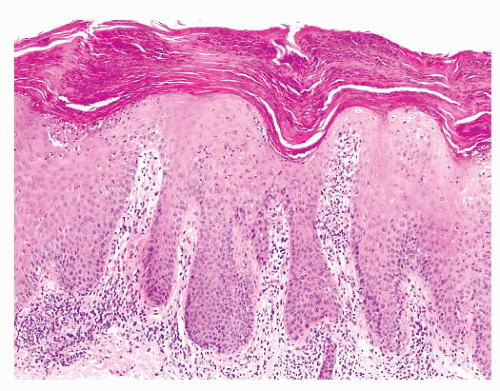 FIGURE 1.5 Psoriasis vulgaris. Epidermal parakeratosis with intracorneal neutrophils, hypogranulosis, and regular psoriasiform acanthosis with suprapapillary plate thinning. Vascularity is increased in the dermal papillae. A perivascular lymphocytic inflammatory infiltrate is present in the papillary dermis. |
another lichenoid disease. The epidermal granular layer often shows focal “wedge-shaped” hypergranulosis. The irregularity of the lichenoid interface change results in the “sawtooth” appearance of the basement membrane zone. Colloid bodies range from rare to abundant. Artifactual cleft formation (Max-Joseph space) between the epidermis and papillary dermis is common, and frank hemorrhagic subepidermal bullae may occasionally be seen. The inflammatory infiltrate in lichen planus is superficial, typically moderate to dense, predominantly lymphocytic, and displays a bandlike distribution closely approximating the epidermis. Melanophages may be abundant, especially in lesions involving darkly pigmented skin (34).
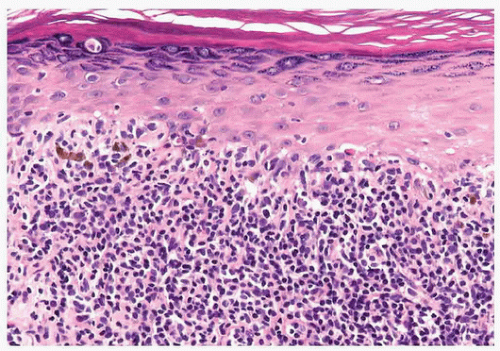 FIGURE 1.6 Lichen planus. Epidermal hypergranulosis, lichenoid interface alteration with “sawtooth” remodeling of the basement membrane zone. A superficial, dense, bandlike lymphocytic inflammatory infiltrate closely approximating the epidermis is present in the dermis. |
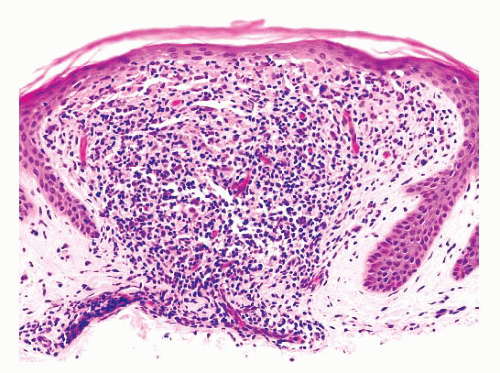 FIGURE 1.7 Lichen nitidus. The epidermis has a “clawlike” configuration with elongated rete. A delineated, lymphohistiocytic inflammatory infiltrate is present in the papillary dermal papilla. |
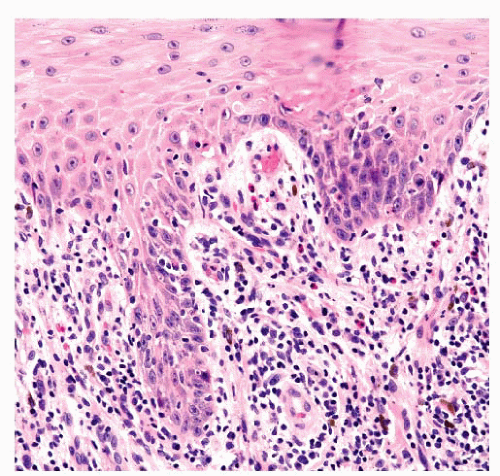 FIGURE 1.8 Lichenoid drug eruption. Epidermal interface alteration and eosinophils in the inflammatory infiltrate provide a clue to the diagnosis of this type of lichenoid interface dermatitis. Epidermal parakeratosis is typically present. |
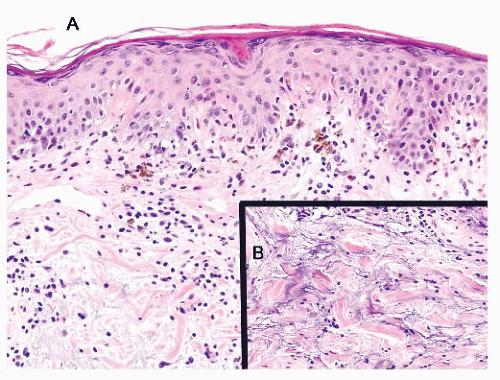 FIGURE 1.9 Discoid lupus erythematosus. (A) Vacuolar epidermal interface alteration is present at the dermal-epidermal junction. A mild lymphocytic inflammatory infiltrate with admixed melanophages are present in the papillary dermis. (B) Increased interstitial dermal mucin in the reticular dermis. |
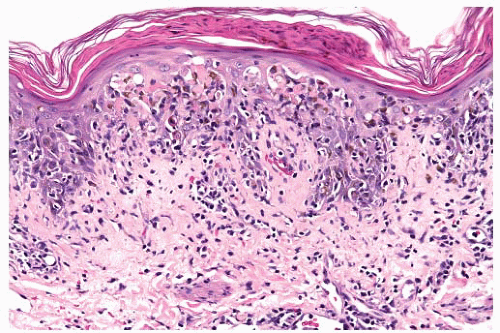 FIGURE 1.10 Pityriasis lichenoides et varioliformis acuta. Sharply demarcated epidermal parakeratosis, spongiosis, vacuolar interface alteration with epidermal necrosis, and lymphocytic exocytosis. A superficial dermal lymphocytic inflammatory infiltrate. |
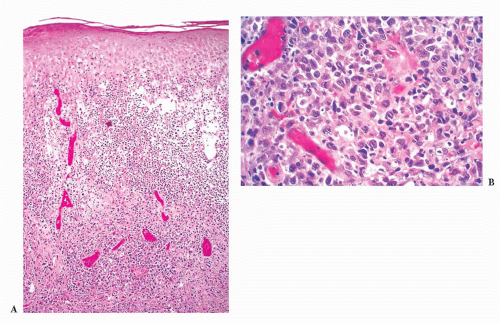 FIGURE 1.11 Lymphomatoid papulosis. (A) A dense dermal lymphocytic infiltrate. The epidermal and dermal alterations often resemble pityriasis lichenoides et varioliformis acuta or pityriasis lichenoides chronica. (B) Under higher magnification, large, atypical lymphocytes with irregularly shaped nuclei are seen. These atypical lymphocytes are CD30-positive and closely resemble atypical lymphocytes in cutaneous lymphomas. |
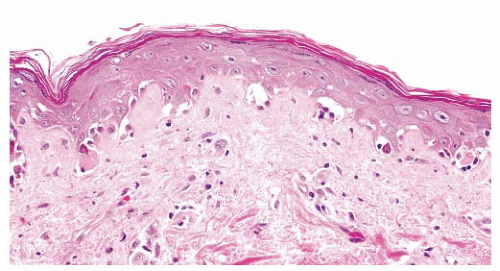 FIGURE 1.12 Acute graft-versus-host disease. Vacuolar epidermal interface alteration with dyskeratotic keratinocytes and a sparse lymphocytic inflammatory infiltrate. |
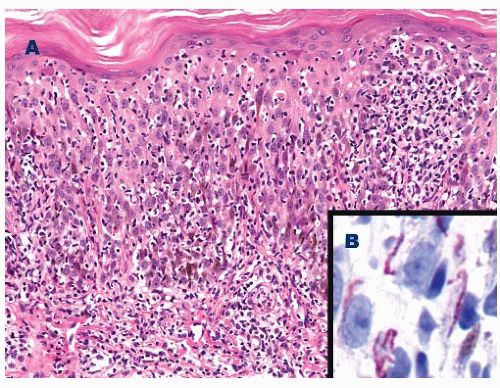 FIGURE 1.13 Secondary syphilis. (A) Irregular psoriasiform epidermal changes and a lichenoid mixed inflammatory infiltrate with prominent exocytosis, plasma cells, and focal vacuolar epidermal interface alteration. (B) Treponemal immunohistochemistry demonstrates spirochete organisms in the epidermis. |
generally the preferred technique to demonstrate spirochete organisms in histologic sections (64).
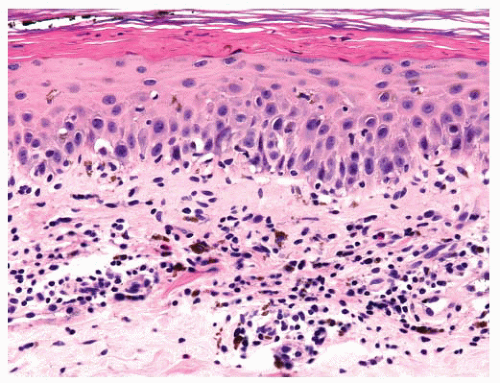 FIGURE 1.14 Fixed drug eruption. Focal vacuolar epidermal interface alteration and a perivascular lymphocytic inflammatory infiltrate. Eosinophils and melanophages are typically present in the papillary dermis. |
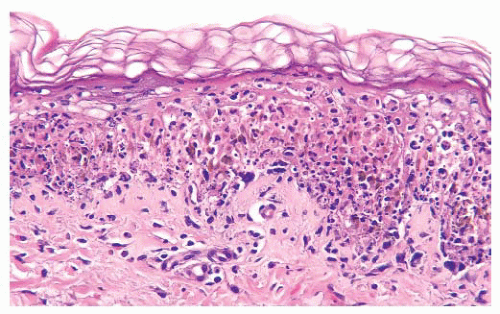 FIGURE 1.15 Erythema multiforme. Prominent vacuolar epidermal interface alteration with associated dyskeratotic keratinocytes and a sparse to mild lymphocytic inflammatory infiltrate. |
shows extensive vacuolar interface alteration, often with fullthickness necrosis and subepidermal bullae (Fig. 1.16). The inflammatory cell component is generally sparse and predominantly lymphocytic.
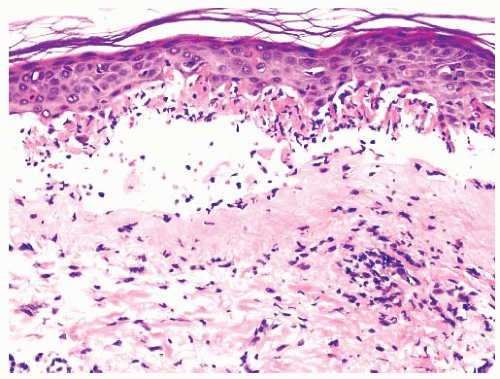 FIGURE 1.16 Toxic epidermal necrosis. Extensive vacuolar epidermal interface alteration with epidermal necrosis and subepidermal blister. A sparse lymphocytic inflammatory infiltrate is present in the dermis. |
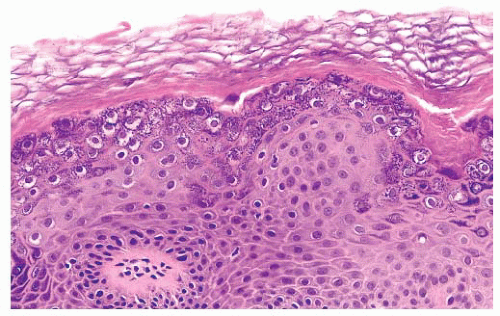 FIGURE 1.17 Verruca vulgaris. Epidermal hypergranulosis and perinuclear clearing in keratinocytes within the granular layer. |
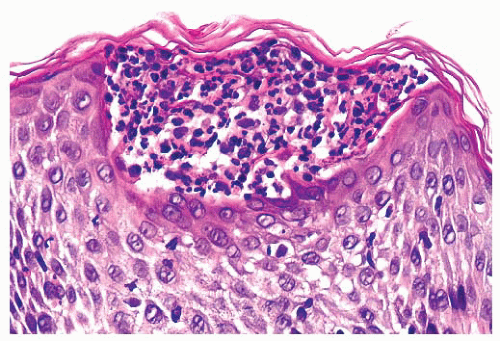 FIGURE 1.18 Subcorneal pustular dermatosis. A unilocular subcorneal aggregate of neutrophils. |
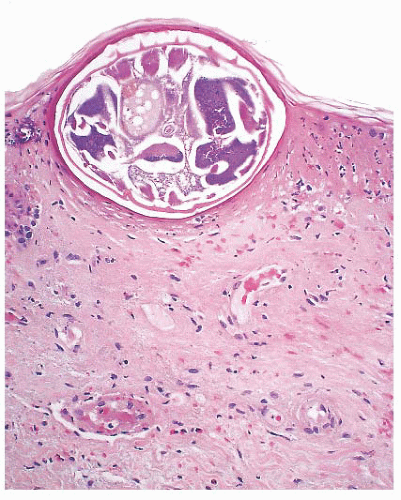 FIGURE 1.19 Scabies. Mite body parts in a subcorneal burrow. |
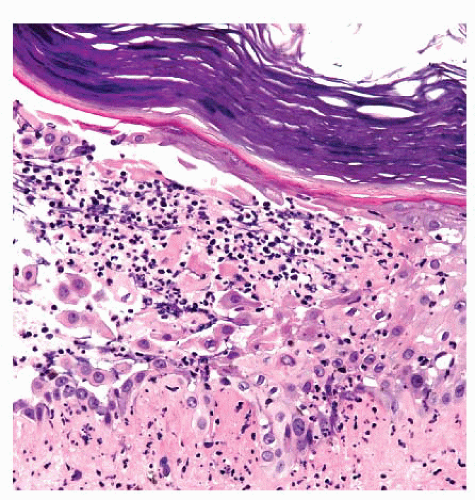 FIGURE 1.20 Bullous impetigo. Subcorneal epidermal bulla with acantholysis and a neutrophilic inflammatory infiltrate in the blister space. |
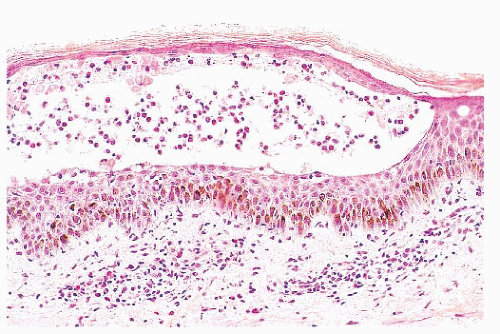 FIGURE 1.21 Pemphigus foliaceus. A subcorneal epidermal bulla with rare acantholytic keratinocytes and a mixed inflammatory infiltrate with eosinophils in the blister space. |
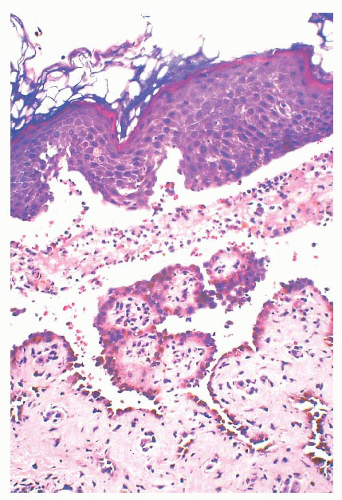 FIGURE 1.22 Pemphigus vulgaris. Suprabasilar epidermal bulla with prominent acantholysis and a mixed dermal inflammatory infiltrate with eosinophils. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


