Patient Story
A 27-year-old woman complains of 2 days of sore throat, fever, and chills. She is unable to swallow anything other than liquids because of severe odynophagia. She denies any congestion or cough. On examination, she has bilateral tonsillar erythema and exudate (Figure 35-1). Her anterior cervical lymph nodes are tender. Based on the presence of fever, absence of cough, tender lymphadenopathy, and tonsillar exudate, she is diagnosed with a high probability of group A β-hemolytic Streptococcus (GABHS) pharyngitis and prescribed antibiotics.

Introduction
Pharyngitis is inflammation of the pharyngeal tissues, and is usually associated with pain. The complaint of “sore throat” is a common one in the primary care office, and can be accompanied by other symptoms and signs including throat scratchiness, fever, headache, malaise, rash, joint and muscle pains, and swollen lymph nodes.
Epidemiology
- Pharyngitis accounts for 1% of primary care visits.1
- Viral infections account for an estimated 60% to 90% of cases of pharyngitis.
- Bacterial infections are responsible for between 5% and 30% of pharyngitis cases, depending upon the age of the population and the season.
- The GABHS accounts for 5% to 10% of pharyngitis in adults and 15% to 30% in children.2 Up to 38% of cases of tonsillitis are because of GABHS.
- Highest prevalence in winter.
- Highest incidence in children between the ages of 4 and 7 years.
- Acute rheumatic fever is currently rare in the United States.
- Up to 14% of deep neck infections result from pharyngitis.3
Etiology and Pathophysiology
- Some viruses, such as adenovirus, cause inflammation of the pharyngeal mucosa by direct invasion of the mucosa or secondary to suprapharyngeal secretions.4 Other viruses, such as rhinovirus, cause pain through stimulation of pain nerve endings by mediators, such as bradykinin.
- The GABHS releases exotoxins and proteases. Erythrogenic exotoxins are responsible for the development of the scarlatiniform exanthem (Figure 35-2). 5 Secondary antibody formation because of cross-reactivity may result in rheumatic fever and valvular heart disease.6 Antigen-antibody complexes may lead to acute poststreptococcal glomerulonephritis.
- Untreated GABHS pharyngitis can result in suppurative complications including bacteremia, otitis media, meningitis, mastoiditis, cervical lymphadenitis, endocarditis, pneumonia, or peritonsillar abscess formation (Figure 35-3). Nonsuppurative complications include rheumatic fever and poststreptococcal glomerulonephritis.



Diagnosis
- Rhinorrhea and cough are more consistent with viral etiology.
- Rapid onset odynophagia, tonsillar exudates, anterior cervical lymphadenopathy, and fever are consistent with streptococcal pharyngitis.
- Not all tonsillar exudates are caused by streptococcal pharyngitis. Mononucleosis and other viral pharyngitis can cause tonsillar exudates (Figures 35-4 and 35-5). The positive predictive value for tonsillar exudate in strep throat is only 31%; that is, 69% of patients with tonsillar exudate will have a nonstreptococcal cause.
- Para- and supratonsillar edema with medial and/or anterior displacement of the involved tonsil and uvular displacement to the contralateral side suggest peritonsillar abscess (Figure 35-3). Trismus and anterior cervical lymphadenopathy with severe tenderness to palpation are additional findings.
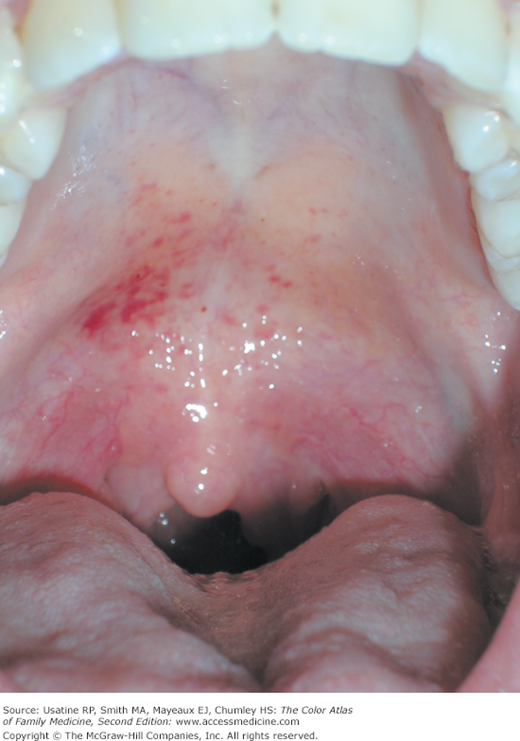
- Palatal petechiae can be seen in all types of pharyngitis (Figure 35-6).
- A sandpaper rash is suggestive of scarlet fever (Figure 35-2, and Chapter 34, Scarlet Fever and Strawberry Tongue).
- Lymphoid hyperplasia can cause a cobblestone pattern on the posterior pharynx or palate from viral infections, gastroesophageal reflux disease (GERD), or allergies (Figure 35-7). Although it usually is more suggestive of a viral infection or allergic rhinitis, lymphoid hyperplasia can be seen in strep pharyngitis (Figure 35-8).
- The following criteria are helpful in the diagnosis of GABHS pharyngitis:7–10
- History of fever or temperature of 38°C (100.4°F) (1 point).
- Absence of cough (1 point).
- Tender anterior cervical lymph nodes (1 point).
- Tonsillar swelling or exudates (1 point).
- Age:
- <15 years (1 point).
- 15 to 45 years (0 points).
- >45 years (−1 point).
- <15 years (1 point).
- History of fever or temperature of 38°C (100.4°F) (1 point).



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


