8 Pharmacoeconomics
While there have been marked gains in life expectancy in those countries which make up the Organization for Economic Co-operation and Development (OECD), health costs have also risen in all of them. The USA spent 16% of its national income (gross domestic product, GDP) on health in 2007, a value considerably greater than many other OECD countries (Fig. 8.1).
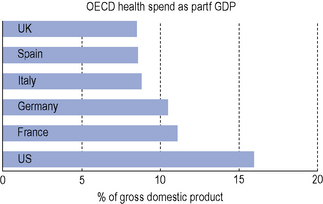
Fig. 8.1 Comparison of health spend as a percentage of gross domestic product in different countries in 2007 (OECD, 2009).
Most OECD countries have seen growth in spending on medicines outstrip growth in total health spending over this period. In the USA and Australia, pharmaceutical spending has increased at more than double the rate of growth in total health spending (OECD, 2009).
There are a number of reasons why prescribing costs are increasing:



