Parasites
Several parasites may be found in the lungs and associated tissues of humans. Of these, only two infect human lungs by preference: Dirofilaria immitis and Paragonimus sp. The remainder are in transit to another organ, in the wrong host or tissue, or disseminated. In this chapter, we illustrate some of the more common parasites that can be encountered in the lung.
Part 1 Dirofilaria
Abida K. Haque
Dirofilaria immitis, the dog heartworm, can infect humans when the infective larva is deposited subcutaneously by an infected mosquito’s bite. The larvae grow into immature worms and are carried to the pulmonary circulation, where they become trapped and die, producing pulmonary vascular occlusion and infarction.
Histologic Features
Characteristic histologic lesion shows a circular or wedge-shaped area of coagulative necrosis with a pulmonary artery branch in the center containing the coiled worm, surrounded by granulomatous reaction.
The immature worm measures 100 to 360 μm in diameter, with a thick cuticle (5-25 μm), prominent muscular wall, and inconspicuous lateral chords.
The cuticle projects inward at the lateral chords, forming prominent internal longitudinal ridges.
The worm may not be easily found in some cases and may require deeper levels and elastic stains.
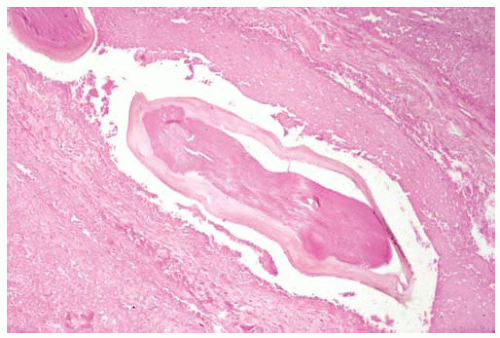 Figure 101.1 The center of an infarct with a pulmonary artery containing a cross-section of Dirofilaria associated with thrombus. |
Part 2 Strongyloides
Abida K. Haque
Infection with Strongyloides is endemic in developing countries, including southern, eastern, and central Europe, and Appalachian United States. Travel to endemic areas can result in acquiring infection. The infection may be latent for years or decades, only becoming active with immunosuppression, particularly with corticosteroid treatment.
S. stercoralis causes lung infection as the larvae migrate through the pulmonary circulation, enter the alveoli through the capillaries, and molt there as part of their life cycle. In immunocompromised individuals, all stages of maturation can be present in the lung, including the filariform and rhabditiform larvae, eggs, and rarely adult worms. Marked tissue eosinophilia with granulomas should alert one to examine carefully for parasites.
Cytologic Features
Filariform larvae may be seen in a background of inflammation, necrosis, and hemorrhage.
Eggs of Strongyloides may be seen in cytologic preparations of sputum specimens.
Histologic Features
The lungs show acute inflammation, necrosis, hemorrhage, and abscesses.
In chronic infection, multiple granulomas with or without larvae in the center are seen in the pulmonary interstitium and alveoli.
Granulomatous inflammation of the airways and rarely the pulmonary vessels may be seen.
The filariform larvae are long and slender (500-600 μm long and 10-16 μm in diameter), and most frequently found in extraintestinal sites; the larvae have a cylindrical esophagus occupying almost half of its length, and four lateral alae.
The rhabditiform larvae (300-380 μm long and 20-25 μm in diameter) are only rarely found in the lungs; the larvae have a short bulbar esophagus and a thin, longer intestine.
The adult females (1.5-10.0 mm long and 30-95 μm in diameter) are found in the small intestine and very rarely in the lungs; the cuticle of the parasite is finely striated, and cross-section may show a muscular esophagus, intestine, ovary, and eggs.
 Figure 101.2 Gross figure showing consolidation with multiple areas of necrotizing bronchopneumonia, some with cavities. |
 Figure 101.3 Cytology figure of sputum showing filariform larva with basophilic nuclei in the posterior two-thirds of the organism. |
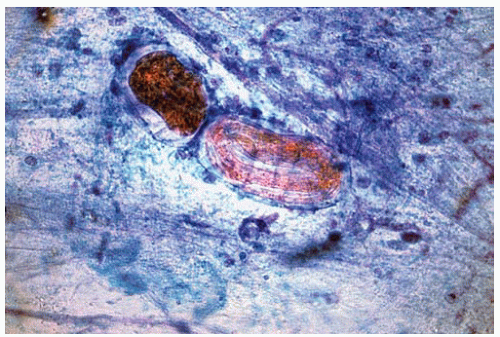 Figure 101.4 Cytology figure of sputum showing eggs of Strongyloides. |
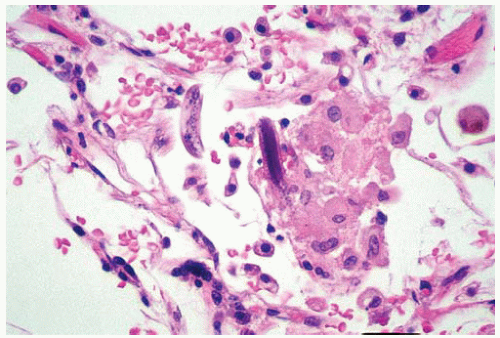 Figure 101.5 High power showing sections of larvae surrounded by macrophages. |
Part 3 Malaria
Judith F. Aronson
Four species of malarial protozoa, Plasmodium, cause human infection: P. vivax, P. malariae, P. ovale, and P. falciparum. P. falciparum causes the most severe form of malaria, including cerebral malaria, which is commonly fatal. During the erythrocytic cycle of parasite replication, human red blood cells become heavily parasitized by trophozoites. Parasitized red
blood cells adhere to microvascular endothelium via knobs on the surface of the infected erythrocytes. This leads to widespread microcirculatory disturbance in virtually all of the visceral organs, including the lung.
blood cells adhere to microvascular endothelium via knobs on the surface of the infected erythrocytes. This leads to widespread microcirculatory disturbance in virtually all of the visceral organs, including the lung.
Histologic Features
Pulmonary congestion is seen, with stasis of parasitized erythrocytes in the capillaries.
Parasitized erythrocytes are recognized by presence of basophilic “ring forms” of the trophozoite and the presence of malarial pigment, the result of hemoglobin digestion by the parasite.
Alveolar septa may display mononuclear infiltrates, composed of monocytes, lymphocytes, and plasma cells.
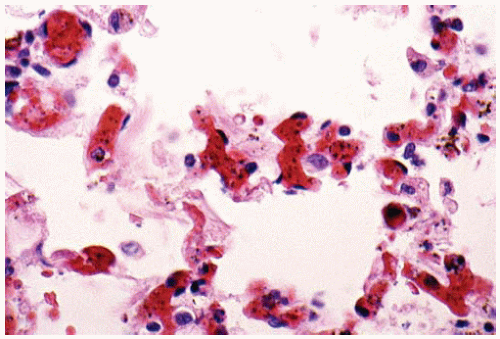 Figure 101.6 Alveolar capillaries containing numerous parasitized red blood cells, from an autopsy of a young, asplenic West African man. |
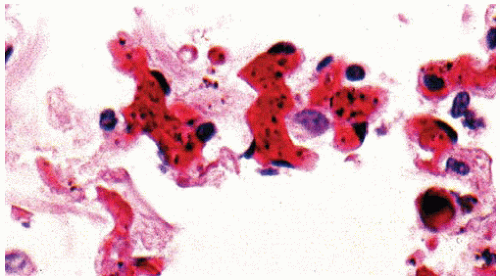 Figure 101.7 Higher power showing alveolar capillaries with parasitized red blood cells. |
Part 4 Toxoplasma
Abida K. Haque
Toxoplasma gondii is an obligatory intracellular protozoan that can parasitize humans, cats, and other mammals. Acute infection is often asymptomatic. Acute infection in immunocompromised subjects or infants results in rapid multiplication of the tachyzoites in host cells. The tachyzoites are contained in a cytoplasmic vacuole, forming tissue cysts measuring 15 to 100 μm. Tachyzoites are crescentic in shape, 4 to 8 μm in length and 2 to 3 μm in width, with one end broader than the other.
Chronic infection is characterized by the presence of infective bradyzoites within tissue cysts. Lung infection is characterized by chronic interstitial pneumonia, but organisms are often difficult to find.
Histologic Features
Interstitial pneumonia with mononuclear infiltrate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


