might merit further attention. Symptomatic intervals as long as 6 years have been noted.16 Two patients reported longterm use of phenothiazines.7,17 One of these patients had an elevated serum prolactin level,7 and the papillary epithelium in the other case17 exhibited secretory changes.
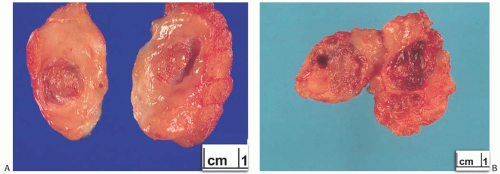 FIG. 5.1. Papilloma. Gross appearance of three lesions. A: Intracystic papilloma. B: Solid intracystic papilloma virtually filling the cyst lumen. C: An everted cystic multinodular papilloma from a 17-year-old girl. D: A histologic whole mount of a tumor similar to the one in (B). |
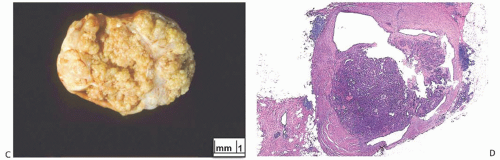 FIG. 5.1. (Continued) |
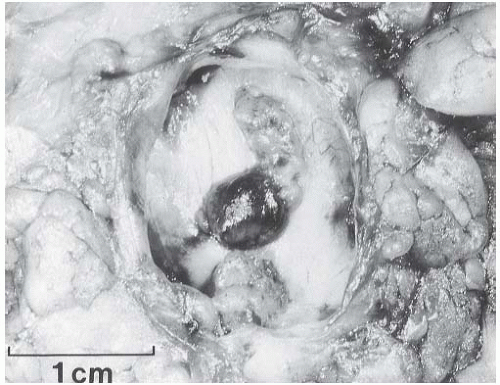 FIG. 5.2. Papilloma. Gross appearance of an intracystic papilloma consisting of two mural nodules. The cyst wall is a distinct fibrous membrane with a smooth inner surface. |
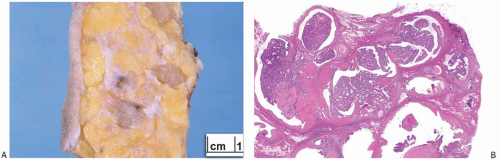 FIG. 5.3. Multiple intraductal papillomas. A: Gross specimen showing multiple papillomas. The two largest lesions are solid, tan tumors. A small cystic papilloma is visible in the center. B: A cluster of small intraductal papillomas. |
both processes, resulting in fusion of the papillary fronds (Fig. 5.6). The most exaggerated form of this process is the solid intraductal papilloma, in which virtually all the space between fibrovascular stalks is filled by solid sheets of proliferative ductal epithelial cells. More often, secondary lumens are formed within the hyperplastic epithelium, resulting in irregular microlumens, micropapillary fronds, focal solid areas, or heterogeneous combinations of these patterns (Fig. 5.7).
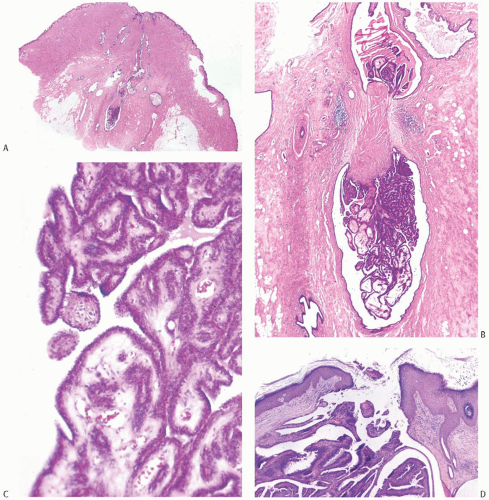 FIG. 5.4. Papilloma of lactiferous duct. A,B: A dumbbell-shaped papilloma with a central zone of fibrosis. C: The papillary fronds are composed of somewhat edematous fibrovascular stroma with a thin layer of epithelium on the surface. Similar epithelium lines the lumen of the dilated duct. D: A papilloma at the level of a lactiferous duct orifice. E: Florid epithelial hyperplasia in a lactiferous duct papilloma. |
papillary configuration, apocrine metaplasia is usually cytologically bland, but apocrine atypia manifested by nuclear pleomorphism and cytoplasmic clearing can be seen in sclerosing papillary tumors. This is especially common when sclerosing adenosis (SA) is incorporated into a papilloma.
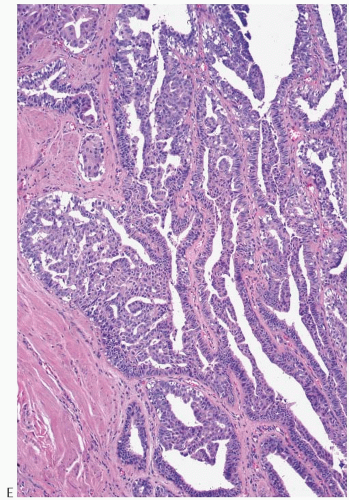 FIG. 5.4. (Continued) |
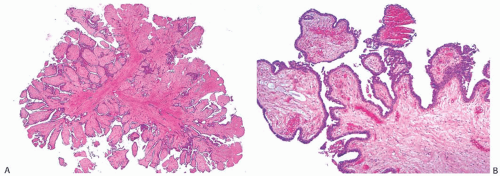 FIG. 5.5. Papilloma. A: This papilloma has dense collagenous stroma. B: Epithelium on the surfaces of the fronds is thin. C: A thin layer of cuboidal and columnar epithelial cells overlies a continuous layer of myoepithelial cells (arrows). D: Slight epithelial hyperplasia at the surface of one papillary frond. |
actin, calponin, myosin heavy chain, CD10, p63, and CK5/6 (Fig. 5.13). All of these proteins except p63 are cytoplasmic markers, which vary in their proclivity to react with stromal cells. The p63 immunostain localizes in myoepithelial cell nuclei and rarely in the nuclei of epithelial cells in a papillary lesion.28 Cross-reactivity in stromal cells is not observed. For this reason, it is preferable to include a stain for p63 among those chosen to detect myoepithelial cells. The myoepithelium may become noticeably attenuated and focally undetectable by immunostains in regions of sclerosis in a papilloma. The focal absence of immunoreactive myoepithelium, by itself, is not diagnostic of carcinoma in this setting. When there is marked hyperplasia of myoepithelial cells in a benign papillary tumor, the differential diagnosis includes AME.
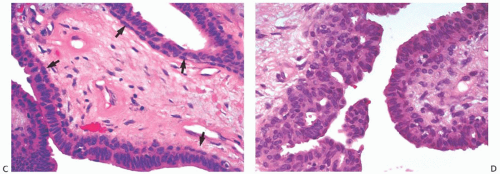 FIG. 5.5. (Continued) |
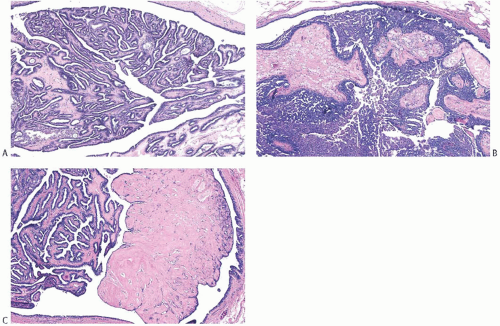 FIG. 5.6. Papillomas. Histologic appearances of three different tumors. A: Papilloma with simple epithelium and complex glands. B: Papilloma with prominent epithelial hyperplasia. C: Papilloma with complex glands and a discrete nodular area of sclerosis that distorts the underlying papillary architecture. |
sometimes associated with displaced epithelium. Spontaneous infarction usually involves superficial portions of a papilloma. Rarely, the entire lesion is infarcted either spontaneously or as a consequence of a biopsy. The underlying structure of a fully infarcted papilloma can be demonstrated with a reticulin stain. In some infarcted lesions in which degeneration is not advanced, the structure of the epithelium can be displayed more clearly with immunostains such as cytokeratin (CK) and p63.29 There is no procedure for reliably distinguishing between the completely infarcted epithelium of a papilloma and that of a papillary carcinoma. However, if myoepithelium can be demonstrated in the infarcted tissue, the tumor is more likely to be a papilloma than a papillary carcinoma. Cytologic atypia is commonly found in the partially degenerated epithelium of a papilloma in the vicinity of infarcts. The atypia is usually manifested by nuclear hyperchromasia and pleomorphism. These cytologic abnormalities may lead to an erroneous diagnosis of carcinoma in the fine-needle aspiration (FNA) specimen from an infarcted papilloma30,31 or in a needle core biopsy specimen.
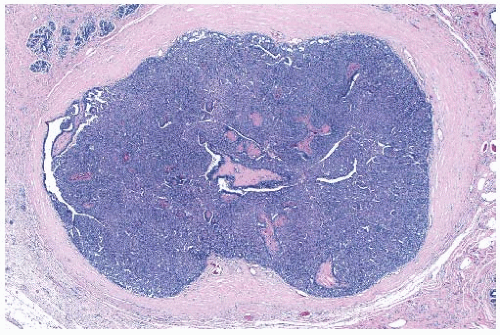 FIG. 5.7. Papilloma. Florid ductal hyperplasia obscures the papillary architecture of this solid papilloma. |
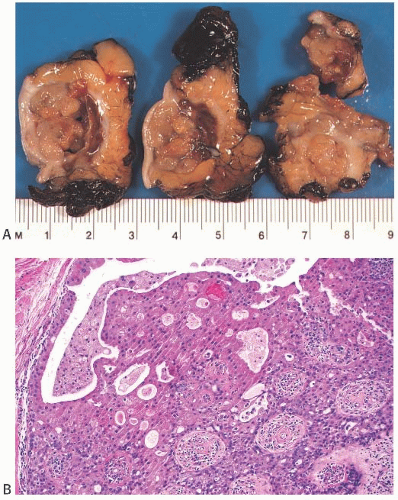 FIG. 5.8. Papilloma with apocrine metaplasia. A: The light brown color of this cystic papillary lesion is typical of tumors with extensive apocrine metaplasia. B: Hyperplastic apocrine epithelium on the surface of a papillary frond. |
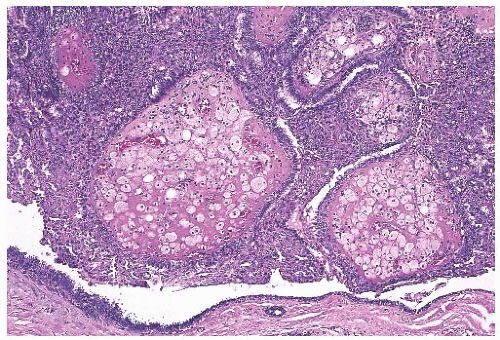 FIG. 5.9. Papilloma with stromal histiocytes. The fibrovascular stroma is prominent as a result of accumulated histiocytes in a papilloma, which nearly fills a cystically dilated duct. Part of the duct wall is seen at the bottom of the image. |
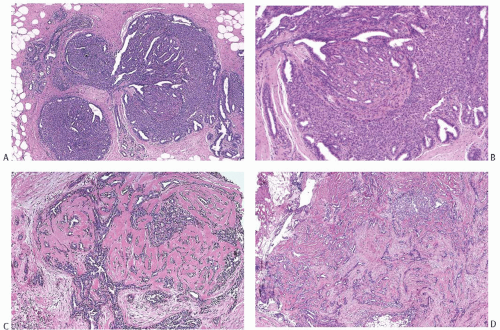 FIG. 5.10. Papilloma with stromal sclerosis. A: A trilobed solid papilloma showing early central sclerosis. B: Florid duct hyperplasia and adenosis in the lesion shown in (A). C: Well-developed sclerosis is present throughout this papilloma. D: Sclerotic stroma is uniformly distributed in this lesion. |
specimens of papillary lesions by Masood et al.,40 3 of 21 tumors interpreted as benign papillary lesions proved to be micropapillary ductal carcinoma in situ (DCIS) upon study of an excision specimen. Immunostaining may help in the diagnosis of FNA specimens of papillary breast tumors. Chang et al.41 reported that the percentage of Ki67-positive cells was significantly higher in papillary carcinomas (21.0 ± 19.23%) than in papillomas (6.23 ± 7.25%). These investigators did not find cyclin-D1 reactivity to be a useful differential feature. Staining of cell-block preparations for calponin to reveal myoepithelial cells can provide diagnostic information in certain cases.42 For further discussion, see Chapter 14.
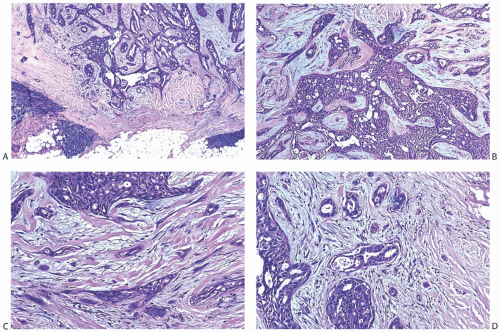 FIG. 5.11. Papilloma with stromal sclerosis. Images are from one tumor. A: The border of the lesion is circumscribed. Note the collections of lymphocytes. B: An area near the center of the lesion showing residual papilloma with fenestrated epithelium. C: Attenuated epithelium is distributed between layers of myofibroblasts and collagen within the tumor. D: This image from the periphery of the lesion shows rounded groups of cells and isolated cells, a characteristic finding at the edges of a papilloma with sclerosis. |
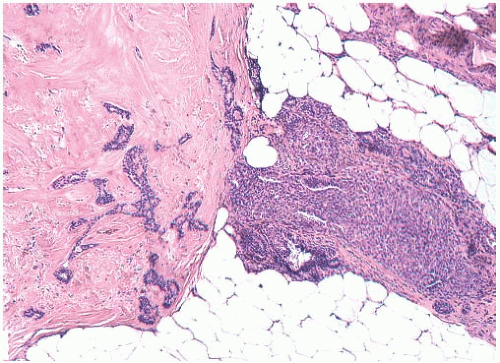 FIG. 5.12. Papilloma with extreme stromal sclerosis. The main tumor is almost entirely effaced by collagenized stroma. An intraductal papilloma persists in a peripheral duct. |
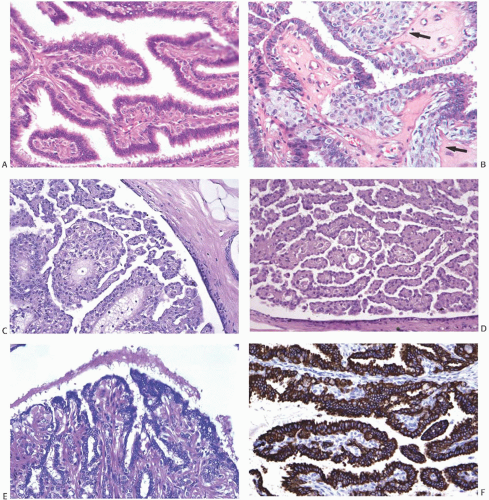 FIG. 5.13. Myoepithelial cell hyperplasia. A: Hyperplastic myoepithelial cells forming an expanded zone beneath the thin epithelium. B: The myoepithelial cells have an epithelioid phenotype (arrows). C,D: Myoepithelial cells with an epithelial phenotype are markedly hyperplastic in these papillomas. The epithelium is reduced to a thin layer of flat cells overlying the multilayered myoepithelium. E: A papilloma in which the myoepithelial cells have a striking myoid phenotype and resemble smooth muscle. F: The AE1/AE3 immunostain is reactive in the epithelium but not in the myoepithelium. G: The myoepithelium is immunoreactive for myosin heavy chain, which shows no reactivity in the epithelium. H: Clusters of epithelioid myoepithelial cells resemble lobular carcinoma in the stroma of this papilloma. I: Reactivity for E-cadherin in the epithelial and myoepithelial cells is shown. Lobular carcinoma would be E-cadherin negative. |
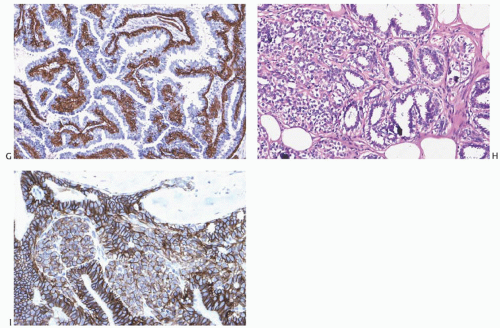 FIG. 5.13. (Continued) |
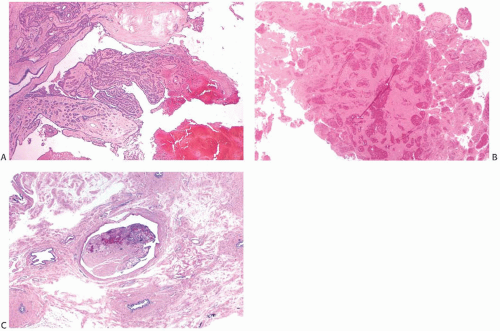 FIG. 5.14. Infarcted papilloma. A: Low-magnification view of infarction in the apical portion of a papilloma. B: This papillary lesion is entirely infarcted. C: A partly infarcted and sclerotic intraductal papilloma. |
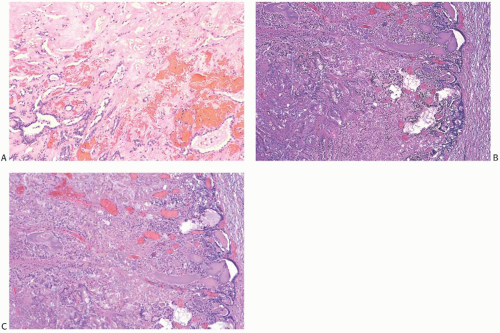 FIG. 5.15. Infarcted papillary tumors. A: Hemorrhage is present at the border of the infarcted zone (above) in a sclerosing papilloma. B,C: The ghost architecture of this papillary lesion is visible (left), and a thin zone of residual viable epithelium is present at the periphery (right). This was probably a solid papilloma. |
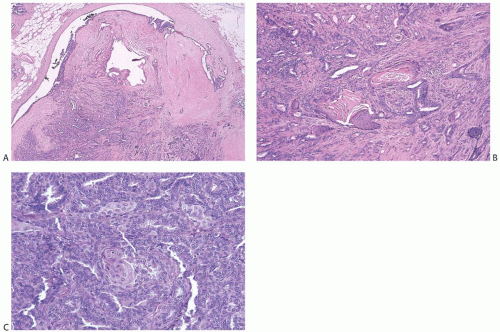 FIG. 5.16. Papilloma with squamous metaplasia. A,B: An intracystic sclerosing papilloma with focal squamous metaplasia. C: A small cluster of cells exhibiting squamous differentiation is present in the epithelium of this florid papilloma. |
TABLE 5.1 Core Biopsy and Excision of Benign Intraductal Papillomaa: A Selected Literature Review | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cytoplasmic organelles include rough endoplasmic reticulum, free ribosomes, Golgi apparatus, and mitochondria. The cytoplasm contains variable numbers of intermediate filament, lipid droplets, lysosomes, and dense secretory granules. Myoepithelial cells sit between the epithelial cells and the basement membrane. They exhibit polygonal or spindly shapes and possess fusiform nuclei. Myofilaments with dense bodies run parallel to the long axis of the cell, and tonofilaments arranged in thick bundles are arranged in a curvilinear pattern. The basal aspects of the myoepithelial cells often display scalloping. Rare cells display features of both epithelial and myoepithelial cells. A thick basement membrane, which often exhibits splitting and reduplication, separates the epithelium from the stroma.
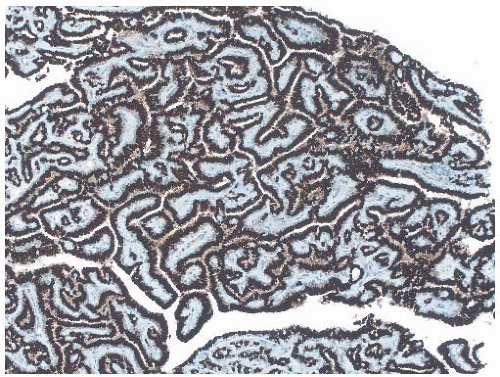 FIG. 5.17. Estrogen receptors. Immunoreactivity for ER is present in virtually all the epithelial cells. |
or invasive carcinoma in either breast was 4.6% for patients with a papilloma without atypia and 13% for patients with a papilloma with atypia.
TABLE 5.2 Intraductal Papilloma and Carcinoma: A Selected Literature Review | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
factors, rather than a reparative process. In this regard, Jacobs et al.90 compared the “expression of factors involved in vascular stroma formation” in radial scars with invasive carcinomas. When compared with normal breast tissue, the stroma of both radial scars and invasive carcinomas displayed increased vascularity as well as “focally increased expression” of mRNA for collagen type IV, total fibronectin, vascular permeability factor/vascular endothelial growth factor, and other markers. These results provided molecular confirmation of the presence of a vasoproliferative process in both radial scars and invasive carcinomas; however, they did not identify the mechanism by which this process occurs, nor did they necessarily indicate that the same mechanism is involved in both lesions. The term radial sclerosing lesion, used here, is preferable because it describes the mammographic and histopathologic appearance of the process without implying histogenesis, and it is sufficiently nonspecific to encompass the many histologic variants included in this category. RSLs are discussed in this chapter devoted to benign papillary tumors because a substantial proportion has a component of papillary ductal proliferation.
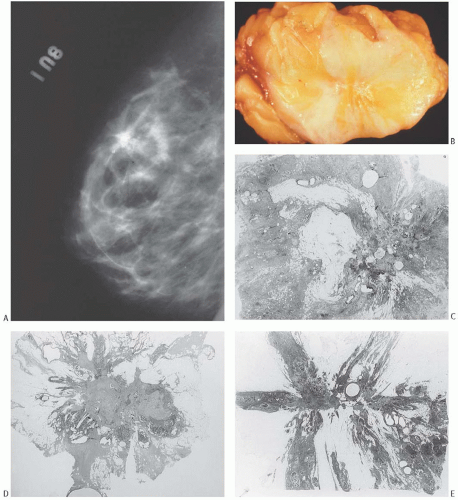 FIG. 5.18. Radial sclerosing lesion. A: Mammogram showing a RSL with a large calcification. B: Gross appearance of the lesion seen in (A). The RSL is the stellate whitish lesion near the center of the tissue. C-F: Whole-mount histologic sections showing different structural patterns. Relatively ill-defined lesion with multiple cysts (C). Asymmetric, oval lesion with dense central fibrosis. A proliferative component and cysts are present around half of the circumference (D). Lesion with a stellate pattern (E). Ovoid tumor with a contour that is partly smooth and partly stellate (F). |
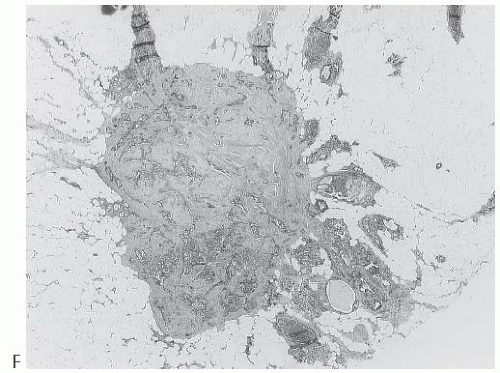 FIG. 5.18. (Continued) |
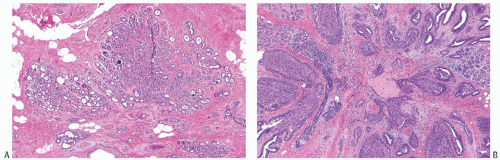 FIG. 5.19. Radial sclerosing lesions, elastosis. A: Foci of SA radiate from the elastotic core. B: Florid duct hyperplasia around an elastotic core. |
proliferative foci are distributed in multiple tissue fragments in a needle core biopsy specimen. Care should be taken to avoid an erroneous diagnosis of DCIS or invasive carcinoma in this setting. Myoepithelial cells can be demonstrated around the perimeter of most hyperplastic ducts by using immunostains for p63, CD10, smooth muscle myosin-heavy chain (SMM-HC), or actin. However, in the central part of the lesion, myoepithelium may be substantially attenuated and even undetectable around hyperplastic ducts (Fig. 5.23).
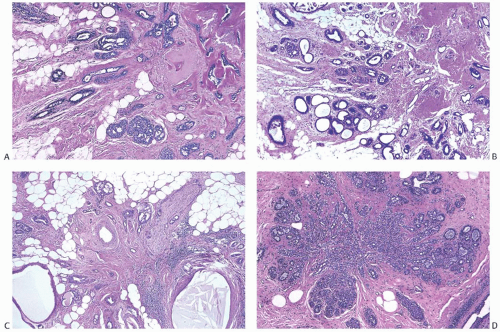 FIG. 5.20. Radial sclerosing lesions. A: The elastotic center is in the upper right corner. Mild ductal hyperplasia is present at the periphery. B: The elastotic center is in the upper right corner. The lesion features adenosis with microcystic dilation of glands. C: A RSL with peripheral apocrine cysts and an entrapped nerve (upper right). D: A RSL composed of SA. |
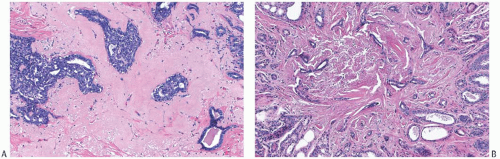 FIG. 5.21. Radial sclerosing lesion. A: Ductal hyperplasia and fibroelastotic stroma. B: Adenosis with a pattern that simulates tubular carcinoma. |
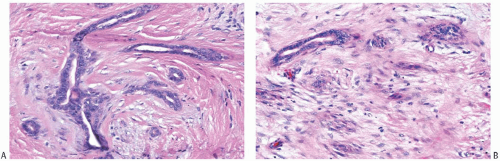 FIG. 5.22. Radial sclerosing lesion simulating invasive carcinoma. A: Irregular ductules in desmoplastic stroma. B: The distinction between epithelial and stromal cells is obscured. |
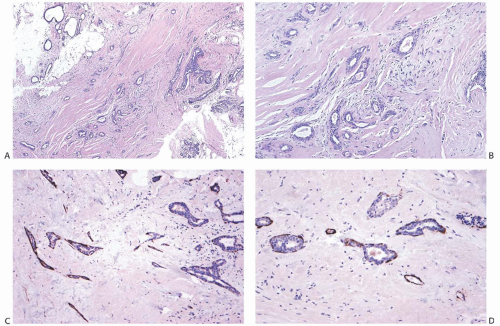 FIG. 5.23. Radial sclerosing lesion, needle core biopsy. A: A low-magnification view of the biopsy sample shows small angular glands in the fibroelastotic stroma. A focus of ductal hyperplasia is present near the right border. This specimen was misinterpreted as tubular carcinoma. B: Angular glands in the myofibroblastic stromal proliferation. C: Actin-positive myoepithelial cells surround these glands in a RSL. D: Incomplete and focally absent SMM-HC immunoreactivity in a RSL. |
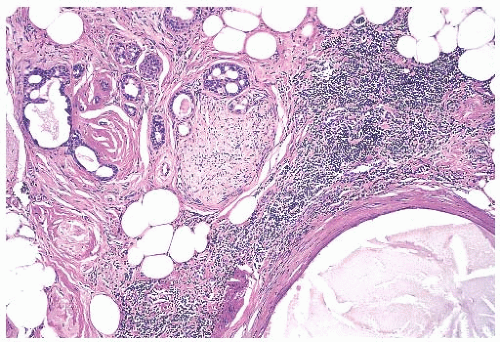 FIG. 5.24. Nerve entrapment in a radial sclerosing lesion. A nerve is shown in the upper center at the periphery of a RSL. Small glands at the perimeter of the perineurium indent the nerve. |
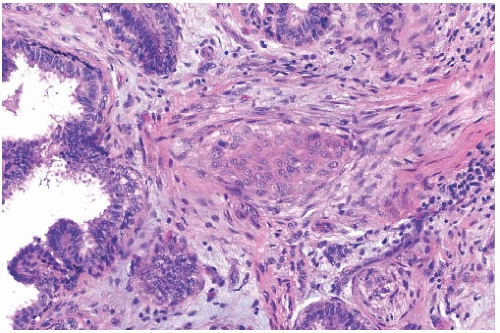 FIG. 5.25. Squamous metaplasia in a radial sclerosing lesion. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


