Ovarian Epithelial-Stromal Tumors. Serous Tumors
Epithelial/Stromal Tumors
The tumors in this category account for approximately two-thirds of all ovarian tumors and for about 90% of all ovarian cancers in the Western world.1,2 Epithelial ovarian tumors are heterogeneous neoplasms that are primarily classified according to cell type into serous, mucinous, endometrioid, clear cell, transitional, and squamous cell tumors.1–3 However, benign counterparts of these cells are not found in the normal ovary and their neoplastic occurrence has long been attributed to müllerian ‘neometaplasia’ of the ovarian surface epithelium (mesothelium), which derives from the celomic epithelium. Specifically, since the celomic epithelium gives rise to the müllerian ducts, it was proposed that, as the surface epithelium becomes malignant, it would acquire the morphologic features of the müllerian duct epithelium; i.e., serous (fallopian tube-like), endometrioid (endometrium-like), and mucinous (endocervical-like). This aberrant differentiation constitutes the basis for ovarian tumor classification. However, even if an origin from the surface epithelium cannot be excluded, there is now compelling evidence that a number of tumors thought to be primary ovarian cancers actually originate in other pelvic organs and involve the ovary secondarily. In fact, it has been discovered that high-grade serous carcinomas (HGSCs) may arise from precursor epithelial lesions in the distal fimbriated end of the fallopian tube,4–10 whereas endometrioid and clear cell carcinomas originate from ovarian endometriosis.11,12 The relative importance of the fallopian tube mucosa compared with the ovarian surface epithelium (mesothelium) in the genesis of high-grade serous ovarian cancers is still a subject of debate. On the other hand, it can be argued that tumors arising in endometriosis are ultimately of endometrial origin. Thus, in some cases, the term ovarian cancer may not be accurate, and it has been suggested that it should be replaced with the terms pelvic or peritoneal cancer. However, given the confusion that might follow in the literature, we think it best to keep the term ovarian cancer until the various possible origins of these diseases are known better.
However, the subdivision of epithelial–stromal tumors that is most important from a clinical viewpoint is their classification into benign, borderline, and carcinoma forms, because it generally correlates with prognosis. This is done according to the amount of tumor cell proliferation, the degree of nuclear atypia, and the presence or absence of stromal invasion.1,2
Borderline Tumors
Borderline tumors (also designated as tumors of low malignant potential) show histologic and cytologic features that are intermediate between those of clearly benign and clearly malignant tumors of the same cell type(s). They exhibit epithelial proliferation greater than that seen in their benign counterparts but an absence of destructive invasion of the stroma or confluent growth, and are associated with a much better prognosis, stage for stage, than that of ovarian carcinomas.2,3,13 Even in the absence of invasiveness within the ovary, borderline tumors of the serous type can either implant on peritoneal surfaces or be associated with independent foci of primary serous peritoneal neoplasia, and, rarely, invasion of the underlying tissues occurs in both circumstances.14–21 Exceptionally, tumors of borderline malignancy spread via lymphatics and blood vessels. In addition, a small number of these tumors are combined with or transform over time into obviously invasive carcinomas.15,19,21 Although favorable in the majority of cases, the biologic behavior of the borderline tumors differs from that of the obviously benign tumors of the same cell type(s). Therefore, the designation ‘tumors of borderline malignancy’ should be kept. Alternative terms such as proliferating, atypical, and atypical proliferative 22 are misleading because they do not imply the malignant potential of a small but significant number of these tumors and discourage complete surgical staging and follow-up of the patients.1–3,13,19 Subdivision of the borderline group into benign and malignant, based on the presence of micropapillary architecture, is artificial since tumors with or without micropapillary pattern may rarely be associated with invasive peritoneal implants and poor outcome. Although the word ‘borderline’ may suggest uncertainty, it accurately describes the ambiguous histologic and biologic features of these neoplasms and remains the most appropriate term. Accordingly, it has been recommended by the World Health Organization (WHO) for the last four decades.3
The distinction between borderline tumors and carcinomas is one of the most common problems in ovarian tumor pathology, yet the literature on borderline tumors is confusing, particularly with regard to their diagnostic features and treatment. Although the WHO3 has recommended the presence or absence of ‘obvious invasion’ of the stroma, most practitioners do not require obvious stromal invasion for the diagnosis of carcinoma if the epithelial cells are malignant cytologically. To promote terminology agreement, the WHO has proposed such tumors be classified as borderline with intraepithelial carcinoma. The extent of the carcinomatous epithelium should be noted in the pathology report.1–3
Carcinomas
Malignant epithelial tumors (carcinomas) are the most common ovarian cancers, accounting for 90% of cases.2,3 Although traditionally referred to as a single entity, ovarian cancer is not a homogeneous disease but rather a group of diseases, each with different morphology and biologic behavior. Currently, based on histopathology, immunohistochemistry, and molecular genetic analysis, at least five main types of ovarian carcinomas are identified: HGSCs (70%), endometrioid carcinomas (10%), clear cell carcinomas (10%), mucinous carcinomas (3 %), and low-grade serous carcinomas (LGSCs; <5%).23,24 These tumors account for 98% of ovarian carcinomas, can be reproducibly diagnosed by light microscopy, and are inherently different diseases, as indicated by differences in epidemiologic and genetic risk factors, precursor lesions, patterns of spread, molecular events during oncogenesis, response to chemotherapy, and prognosis. The fact that one tumor type (HGSCs) accounts for over two-thirds of cases does not justify classifying ovarian carcinomas into only two pathogenetic types, lumping together the other four (endometrioid, clear cell, mucinous, and LGSCs) as ‘type I carcinomas.’25 In fact, the latter tumors are clinically, morphologically, and molecularly distinct diseases that individually bear resemblance neither to HGSCs nor to each other. Thus, classifying ovarian carcinomas into only two pathogenetic types (‘types I and II’)25 appears to be artificial and simplistic.
Benign and Borderline Serous Tumors
In the Western world, serous tumors account for 30–40% of all ovarian tumors. Of these, approximately 70% are benign, 5–10% borderline, and 20–25% carcinomas.1 Borderline and invasive serous tumors together account for about 30% of the non-benign ovarian tumors.
Benign Serous Tumors
Macroscopic Features
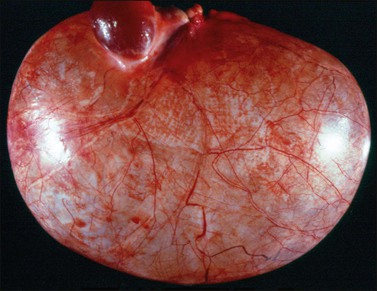
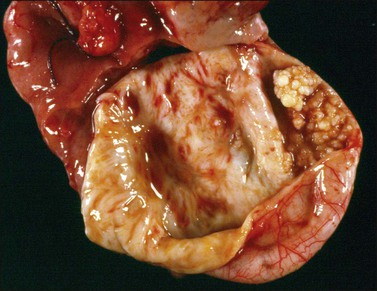
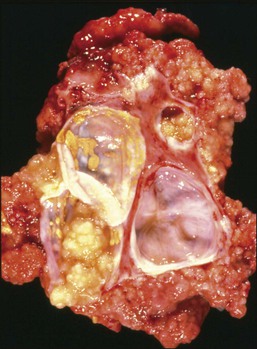
Benign serous tumors are usually endophytic (cystadenomas), but may be exophytic (surface papillomas) or both. Serous cystadenomas are usually unilocular (Figure 25.1) but may be multilocular, and have thin-walled cyst(s) (Figure 25.2) filled with watery or occasionally thin mucinous fluid. They average about 10 cm in size. Customarily, a benign serous tumor is diagnosed only if the lesion is >1 cm in diameter. The cyst(s) may have a smooth inner surface or have polypoid excrescences (Figure 25.3), which are firm if their stroma is fibrous and soft if it is edematous. Serous cystadenomas are bilateral in approximately 10–20% of cases (Figure 25.2).

Microscopic Features
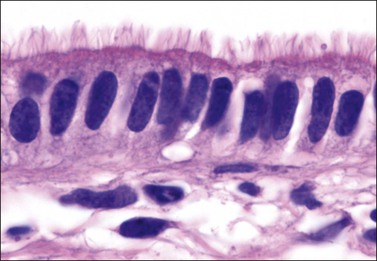
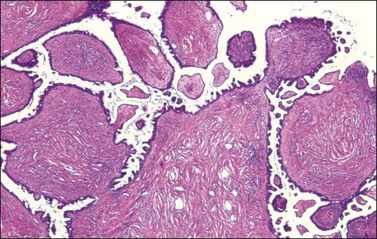
The cysts and polypoid excrescences of benign serous tumors are typically lined by pseudostratified epithelium similar to that of the fallopian tube, which is frequently ciliated (Figure 25.4). Tumors lined entirely by nonciliated cuboidal or columnar epithelium that resembles ovarian surface epithelium are also generally included in the serous category despite their indifferent appearance. The epithelial cells of benign serous tumors may secrete mucin, but, when it is present, it is usually confined to the lumens of cysts and apical portion of the cytoplasm of the epithelial cells. Mitoses are rare. There is no nuclear atypia. Psammoma bodies are infrequent (10%). Papillae when found are composed almost entirely of stroma (Figure 25.5), which may be collagenous or markedly edematous. In adenofibromas and cystadenofibromas, glands and cysts are scattered within a predominantly fibromatous stroma. Otherwise typical benign cystic or surface serous tumors containing minor foci (<10%) consistent with borderline neoplasia (cell stratification and nuclear atypia) are kept in the benign category for clinical purposes.1
Differential Diagnosis
Serous cystadenomas may be confused with rare examples of cystic struma ovarii (Chapter 29), but the latter exhibits at least minor foci of identifiable thyroid follicles in the cyst’s outer wall. Rare rete cystadenomas may simulate serous cystadenomas but, in addition to their hilar location, often show a thick layer of smooth muscle and are lined by cells lacking cilia. Common peritoneal cysts, lined by mesothelial cells, often mimic serous cystadenomas. Serous surface papillary adenofibromas should be distinguished from the common small surface stromal proliferations sometimes seen in adult women. The latter lesions are typically multifocal, have a simple cuboidal epithelial lining, and do not form a mass lesion.
Serous Borderline Tumors
Clinical Features
Serous borderline tumors (SBTs) account for one-fourth to one-third of the non-benign serous tumors.26,27 They are most common in the fourth and fifth decades, with an average patient age of 42 years.21 Although often asymptomatic, the tumor may sometimes present with abdominal enlargement and pain due to rupture or torsion. Approximately 70% are confined to one or both ovaries (stage I) at the time of diagnosis; the remaining tumors have spread within the pelvis (stage II) or upper abdomen (stage III). Only rare cases have extended beyond the abdomen (stage IV) at the time of presentation.19,27 One-third of the stage I tumors are bilateral.27
Macroscopic Features
Serous borderline tumors have one or more cysts that are lined by polypoid excrescences and closely packed finer papillae (endophytic growth) (Figure 25.6). The cysts contain thick mucinous fluid, which does not necessarily indicate the mucinous nature of the tumor. The polypoid excrescences contain fibrous or edematous stroma. Serous borderline cystadenofibromas are firm, white, fibromatous tumors with a cystic component of variable size. In almost 50% of SBTs the papillary growth covers the outer surface of the ovary (serous surface papillary borderline tumor).28 Frequently, both exophytic and endophytic papillary components are present (Figure 25.7). The typical gross features of serous carcinomas, such as friability, hemorrhage, and necrosis, are not seen in SBTs.

Figure 25.6 Serous borderline tumor. Intracystic growth of soft papillary excrescences. (Courtesy of Dr. Jeronimo Forteza, Santiago, Spain.)
Microscopic Features
SBTs show stromal polypoid excrescences, glands, and papillae lined by stratified cuboidal to columnar epithelial cells and ciliated cells resembling those of the fallopian tube (Figures 25.8–25.11). Larger hobnail cells with ample eosinophilic cytoplasm (Figure 25.12) and mesothelial-like cells may also be present. Eosinophilic cells are increased when microinvasion has occurred. The lining epithelial cells show mild to moderate nuclear atypia (rarely severe) and mitoses are rare; therefore, the histologic pattern usually differs from that of carcinoma in situ of other organs. Psammoma bodies are found in about one-fourth of cases. The three most important diagnostic features are (1) arborizing papillae that form increasingly smaller branches ending in clusters of epithelial cells that appear to be detached from the stroma (hierarchical pattern of branching), (2) varying degree of nuclear atypia, and (3) absence of ‘frank’ stromal invasion or solid sheets of tumor with a cribriform pattern.1
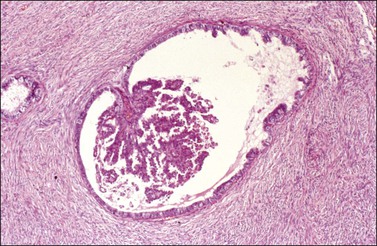
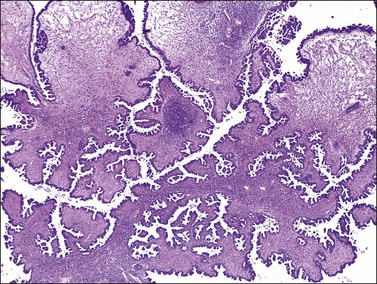
Figure 25.9 Serous borderline tumor, typical pattern. The epithelial papillae show hierarchical and complex branching without stromal invasion. Some papillae have fibroedematous stalks.
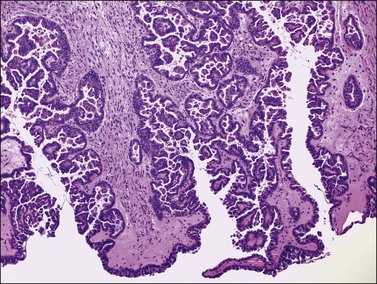
Figure 25.10 Serous borderline tumor, typical pattern. Orderly penetration of the stroma by glands and microcysts with papillae, without stromal reaction. Detachment of small cell nests from the stratified lining epithelium.
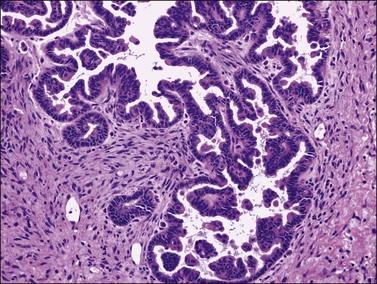
Figure 25.11 Serous borderline tumor, typical pattern. The papillae are lined by stratified cuboidal-to-columnar epithelial cells with hyperchromatic slightly atypical nuclei.
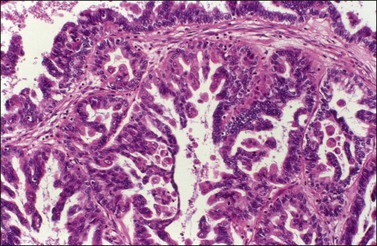
Figure 25.12 Serous borderline tumor. The lining cells are stratified with cellular budding and show moderate atypia. Larger hobnail cells with abundant eosinophilic cytoplasm are seen.
Pseudoinvasion, Autoimplants, and Mesothelial Cell Hyperplasia
Serous borderline tumors often show a relatively complex proliferation of glands and papillae (Figure 25.10). The glands often invaginate into the stroma and, particularly when sectioned tangentially, may appear as if they have invaded the stroma. This pseudoinvasion differs, however, from the destructive stromal invasion of a carcinoma. The stroma about the pseudoinvasion is similar to the stroma elsewhere and the glands have an orderly distribution. In carcinoma, it forms a desmoplastic stroma typically and the neoplastic glands have a more disorderly arrangement. Exceptionally, an SBT implants on itself and may exhibit focal desmoplastic stroma. Autoimplants are sharply circumscribed desmoplastic plaques usually on the outer surface but occasionally on the inner (cystic) surface of the tumor, resembling noninvasive desmoplastic implants on extraovarian peritoneum (Figure 25.13).29 Although the term autoimplant suggests that this lesion might arise by detachment of exophytic SBT and subsequent reattachment to itself, occurrence of this phenomenon has not been confirmed. Autoimplants seem to lack clinical significance. Sometimes, SBTs are partly covered by fibrous adhesions associated with mesothelial hyperplasia, which may be erroneously interpreted as surface borderline tumor or even carcinoma. The mesothelial cells, however, lack nuclear atypia and are typically arranged in a linear fashion (Figure 25.14).
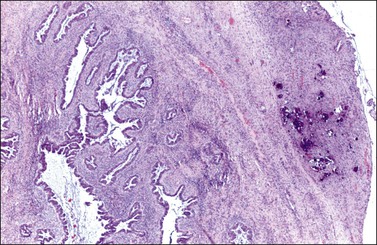
Figure 25.13 Serous borderline tumor with autoimplantation. The upper right corner of the figure shows desmoplastic tissue with numerous psammoma bodies creating an image similar to that of a desmoplastic peritoneal implant. Note the sharp demarcation with the ovarian stroma.
Micropapillary Pattern
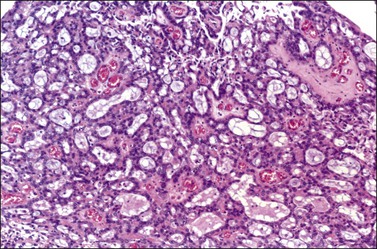
Rarely, SBTs show an exuberant micropapillary (or focal cribriform) proliferation without destructive stromal invasion (Figure 25.15).19 There is a filigree pattern of highly complex micropapillae growing in a nonhierarchical fashion from fibrous stalks (Figure 25.16) composed of stratified nonciliated cuboidal cells with high nuclear to cytoplasmic ratio. Nuclear atypia is only mild with occasional higher grade nuclei present (Figure 25.17). Mitotic figures are rare and no abnormal forms are seen.30 In contrast to the typical SBT, which usually shows variable degrees of cell proliferation and nuclear atypia, the micropapillary or cribriform SBT (Figure 25.18) exhibits a homogeneous and marked degree of cell proliferation and uniform mild nuclear atypia (Figure 25.17). Most micropapillary tumors contain areas of typical SBT, indicating the former’s probable origin.30 When the micropapillary architecture exceeds 5 mm in greatest dimension, it has been recommended to segregate these tumors from the less proliferative SBTs, claiming that they are likely to progress to invasive carcinoma, particularly as invasive peritoneal implants.30 Subsequently, it was required that the ‘micropapillae’ should be five times as long as wide (Figure 25.16).31
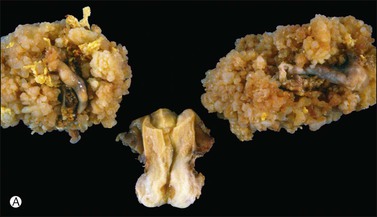
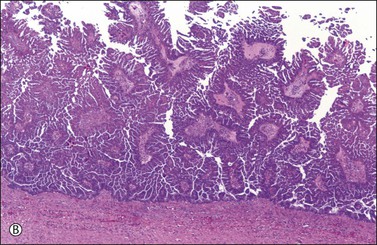
Figure 25.15 (A) Bilateral serous borderline tumor (SBT) with micropapillary proliferation. Both tumors show prominent exophytic papillary growth.19
(Reproduced with permission of Lippincott Williams & Wilkins.)
(B) SBT with micropapillary pattern. The highly complex micropapillae grow in a nonhierarchical fashion from fibrovascular stalks. Stromal invasion is not present.
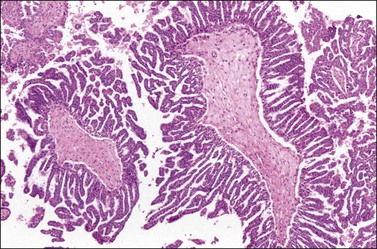
Figure 25.16 Serous borderline tumor with micropapillary pattern (‘Medusa head-like appearance’). Filigree network of small micropapillae, at least five times as long as wide, arising directly from papillary stalks.
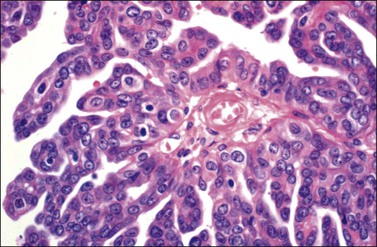
Figure 25.17 Serous borderline tumor with micropapillary pattern. Nuclear atypia is uniform and only moderate (grade 2).
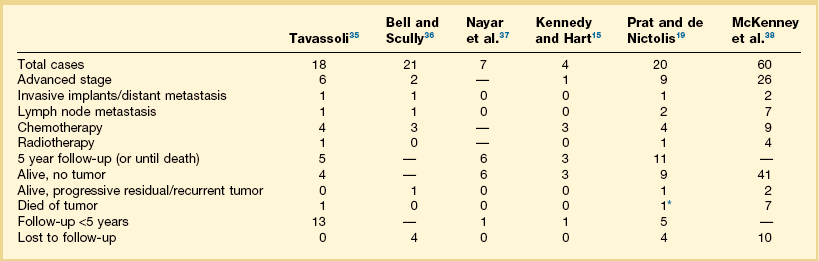
It has been shown that bilaterality, ovarian surface growth, and advanced stage (noninvasive implants) are more common features of micropapillary SBTs than of typical SBTs, but a strong association of the former tumors with invasive implants and poor outcome has been inconsistent. Although in four studies21,31–33 micropapillary SBTs were more frequently associated with invasive implants, micropapillary architecture did not have a significant adverse effect on survival when controlled for implant type. Stage II–III micropapillary SBTs with noninvasive peritoneal implants had the same favorable prognosis as typical SBTs (Table 25.1);16,19,21,30–34 thus, from a prognostic viewpoint, micropapillary SBTs are closer to typical SBTs than to carcinomas. However, although largely noninvasive, serous tumors with prominent micropapillary architecture may contain areas of frank stromal invasion (Figure 25.19); therefore, extensive sampling is indicated in these cases.
Table 25.1
Literature Comparison: Advanced Stage Serous Borderline Tumors with Micropapillary Pattern16,19,21,30–34
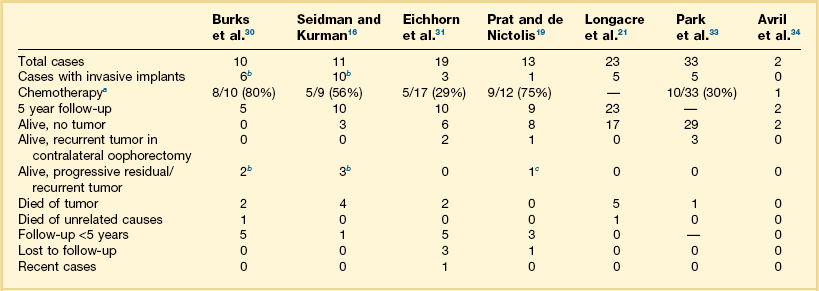
aNumber of patients/number of patients with postoperative treatment information (%).
bIncluding ‘implants with micropapillary’ pattern but without recognizable invasion of underlying tissue.
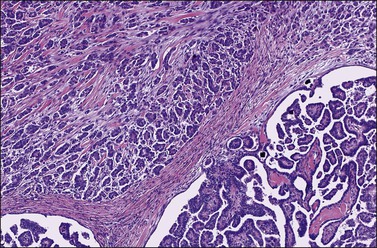
Figure 25.19 Low-grade serous micropapillary carcinoma (upper left) adjacent to serous borderline tumor with micropapillary pattern (lower right). Note the presence of destructive stromal invasion (larger than 10 mm2).
The micropapillary pattern (Figures 25.16 and 25.17), almost always associated with typical SBT, most likely represents a degree of epithelial proliferation intermediate between SBT and LGSCs. By analogy with cervical neoplasia, the difference between typical SBT and micropapillary SBT is like between cervical intraepithelial neoplasia (CIN) 2 and CIN 3. Although the micropapillary pattern in combination with other clinical and pathologic features (i.e., advanced stage, invasive implants, and microinvasion) may be associated with increased risk of disease progression, taken individually, micropapillarity is not a specific predictor of adverse prognosis.21,33,34 Almost all patients dying of recurrent tumor had invasive peritoneal implants, which are the key feature associated with a poor prognosis.
Microinvasion
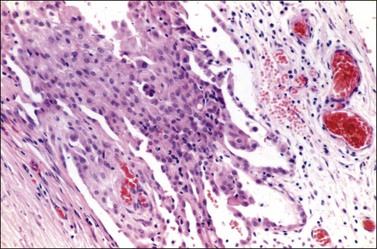
Approximately 10% of otherwise typical SBTs contain one or more discrete foci of stromal microinvasion,15,19,21,35–38 which are made up of single epithelial cells or small clusters of such cells with abundant eosinophilic cytoplasm (Figures 25.20 and 25.21). Often, the cell nests appear surrounded by clefts that separate the epithelium from the stroma (Figures 25.22 and 25.23). These microscopic foci (arbitrarily defined as not exceeding 10 mm2 in area, or 3 mm maximum linear dimension) are typically unassociated with a significant stromal reaction and are easily overlooked on routinely stained sections.1 Cytokeratin (CK) stains help to visualize the invasive epithelial cells (Figure 25.24). Occasionally, foci of lymphatic invasion may be present.36 Several patients with these tumors have been pregnant at the time of diagnosis.38
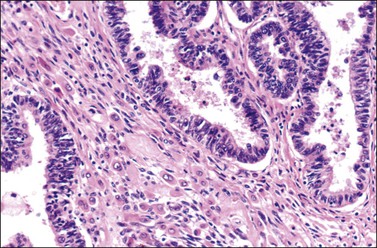
Figure 25.20 Serous borderline tumor with microinvasion. Stromal microinvasion by single epithelial cells and small clusters of such cells with abundant eosinophilic cytoplasm.
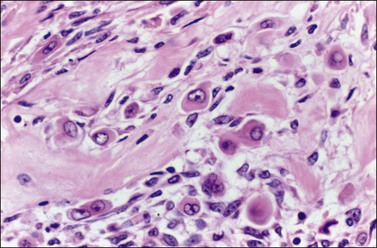
Figure 25.21 Serous borderline tumor with microinvasion. The invasive cells show ample eosinophilic cytoplasm and vesicular nuclei with prominent nucleoli.
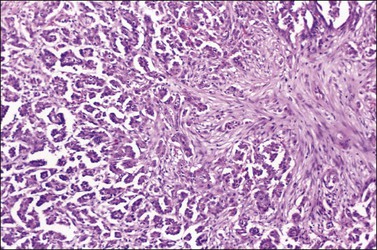
Figure 25.22 Serous borderline tumor with microinvasive carcinoma (2 mm). Destructive invasion of the stroma by malignant-appearing cells and desmoplastic response.
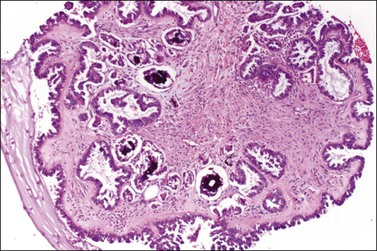
Figure 25.23 Serous borderline tumor with microinvasion. The stroma contains numerous small papillae and clusters of tumor cells surrounded by clefts.
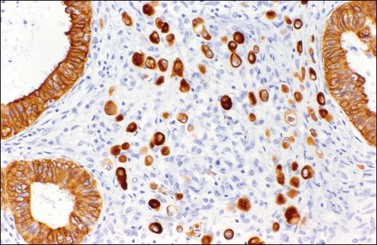
Figure 25.24 Serous borderline tumor with microinvasion. The invasive cells show a strong cytokeratin immunoreaction.
SBTs with microinvasion are associated with a higher frequency of bilaterality, exophytic ovarian surface growth, and advanced stage than typical SBTs lacking microinvasion, yet the rate of invasive implants is similar in both tumor groups.19 At least five studies15,19,35–37 (Table 25.2)15,19,35–38 have confirmed that SBTs with or without microinvasion have a similar prognosis. However, two recent reports21,38 suggested that microinvasion may represent a risk factor for disease progression that is independent of stage and implant status. SBTs with microinvasion (Figures 25.20 and 25.21) should be distinguished from SBTs with microinvasive carcinoma. The latter shows ‘destructive’ invasion of the stroma by malignant-appearing cells and desmoplastic response (Figure 25.22).39 The lesion resembles an invasive peritoneal implant or LGSC. Lymphatic invasion is common and can be demonstrated by D2-40 immunoreaction.40
Peritoneal Implants
One controversial aspect of SBTs is their association in ~30–40% of cases with peritoneal implants.14–21 Implants are found more frequently in patients with tumors that have an exophytic component than in those that do not.28 They rarely present as bulky disease (Figure 25.25), and, in most cases, are either microscopic or small macroscopic (≤1–2 cm) lesions. Their histologic appearance may vary greatly, ranging from foci of benign glandular epithelium resembling endosalpingiosis, to noninvasive papillae, plaques, or nodules of borderline epithelium and stroma, to invasive implants resembling an LGSC.14 Endosalpingiosis, typified by glands, cysts, and occasionally papillae with psammoma bodies, is a benign peritoneal lesion frequently associated with ovarian SBTs (Figure 25.26). It may rarely be the substrate for the development of peritoneal SBTs or carcinomas, but its presence should not change the stage of a synchronous ovarian SBT.
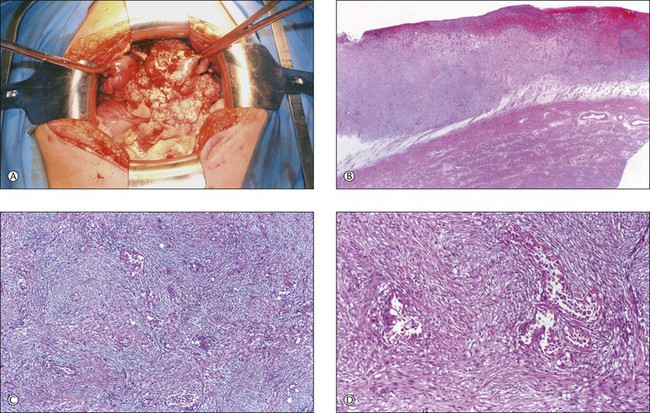
Figure 25.25 (A) Serous borderline tumor (SBT) with noninvasive implants. At laparotomy, the uterus was covered by a soft grayish white and hemorrhagic mass (400 g).
(Courtesy of Dr. Isidre Boguna, Barcelona, Spain.)
(B) Noninvasive desmoplastic implant of SBT. The implant appears plastered upon the uterine serosa without invading the underlying myometrium. The surface of the implant shows hemorrhage and necrosis. (C) Noninvasive desmoplastic implant of SBT. The implant is largely composed of a fibroblastic proliferation which surpasses quantitatively the glandular epithelial component. (D) Noninvasive desmoplastic implant of SBT. Two epithelial glands containing hobnail cells with moderately atypical nuclei are surrounded by dense fibroblastic stroma.
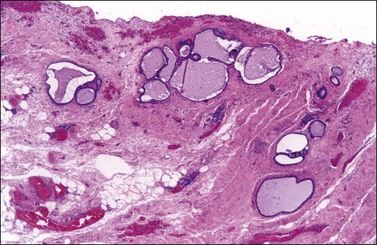
Figure 25.26 Endosalpingiosis. Glands lined by flattened tubal-like epithelium lay in the parametrium.
The peritoneal implants of SBTs have been classified histologically into noninvasive and invasive types with the former further subdivided into epithelial and desmoplastic subtypes.14 The epithelial subtype of noninvasive implants shows papillary proliferations of atypical epithelial cells resembling those of the ovarian SBT (Figure 25.27); they are typically present on the surface of the peritoneum (Figure 25.28)19 or in smoothly contoured subperitoneal invaginations and exhibit little or no stromal reaction.14 In contrast, the desmoplastic subtype of noninvasive implant is largely composed of a stromal proliferation, which is plastered upon serosal surfaces or invaginations between lobules of omental fat (Figures 25.25B–D, 25.29,13 and 25.3043). The stromal reaction surpasses quantitatively the epithelial component of the implant. In late lesions, small glands and papillae lined by atypical serous cells as well as psammoma bodies are entrapped by dense fibroblastic tissue that is often infiltrated by acute and chronic inflammatory cells. Early implants show necrosis with surface fibrin deposition and hemorrhage (Figure 25.3034).14 Invasive implants, which represent approximately 12% of the cases,14,19–21,31 manifest a disorderly infiltration of normal tissues, such as the omentum; in contrast to the well-defined limits of the desmoplastic implants, the invasive implants exhibit irregular borders (Figure 25.31). They usually show a greater epithelial cell population (Figure 25.3219) and resemble histologically a low-grade serous adenocarcinoma (Figure 25.3342); marked cytologic atypia may be present.14 Implants should be sampled extensively since noninvasive and invasive implants may coexist. Also, some implants of serous carcinomas may be noninvasive and simulate the desmoplastic noninvasive implants of SBTs. The former implants, however, usually contain highly atypical epithelial cells.
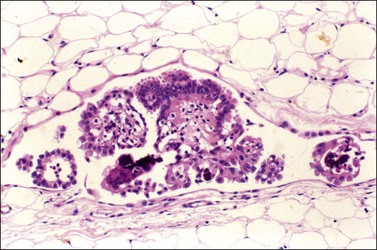
Figure 25.27 Noninvasive epithelial implant of serous borderline tumor within a smoothly contoured invagination of the omental fat. The epithelial proliferation contains calcifications and resembles that of the primary ovarian tumor.
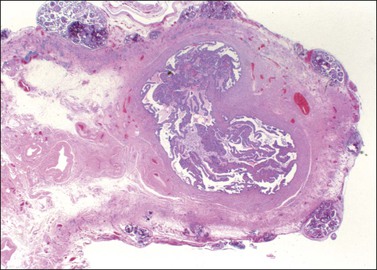
Figure 25.28 Numerous noninvasive epithelial implants of serous borderline tumor on the serosa of the fallopian tube.19 (Reproduced with permission of Lippincott Williams & Wilkins.)
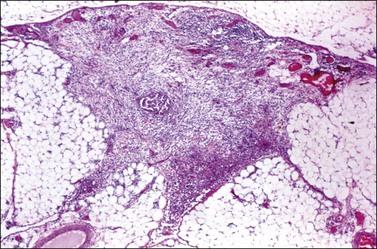
Figure 25.29 Noninvasive desmoplastic implant of serous borderline tumor. The implant invaginates between adjacent lobules of omental fat. Scattered nests of tumor cells are present within a loose fibroblastic stroma.13 (Reproduced with permission of Lippincott Williams & Wilkins.)
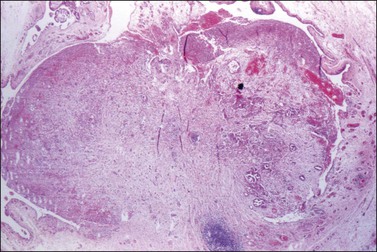
Figure 25.30 Noninvasive desmoplastic implant of serous borderline tumor. The sharply circumscribed nodule is composed predominantly of granulation tissue-like stroma and contains only scattered nests of tumor cells. Foci of hemorrhage and necrosis are seen at the periphery.42 (Reproduced with permission of Lippincott Williams & Wilkins.)
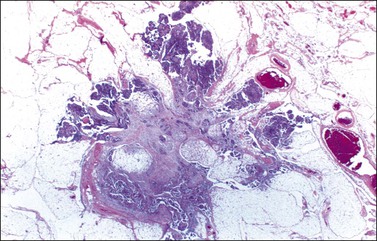
Figure 25.31 Invasive omental implant of serous borderline tumor. The implant is composed predominantly of epithelial cells which invade the adipose tissue in an irregular fashion.
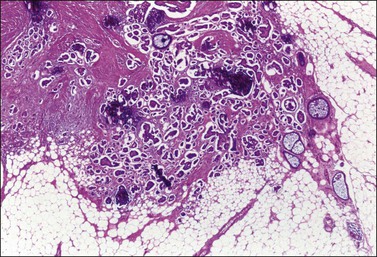
Figure 25.32 Invasive omental implant of serous borderline tumor. The tumor glands and papillae appear disorderly distributed within a desmoplastic (‘collagenized’) stroma and many of them are surrounded by clefts.19 (Reproduced with permission of Lippincott Williams & Wilkins.)
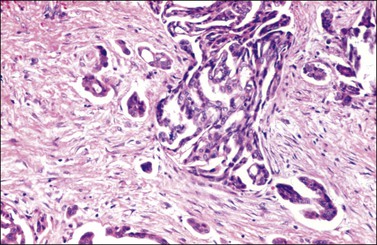
Figure 25.33 Invasive omental implant of serous borderline tumor. The tumor resembles an LGSC. The intervening stroma appears desmoplastic.42 (Reproduced with permission of Lippincott Williams & Wilkins.)
At least 11 studies of SBTs with peritoneal implants (Table 25.3)14–19,21,31,33,34,42–44 have clearly demonstrated that separation of the implants into invasive and noninvasive subtypes carries important prognostic implications. The rare tumors that were fatal were mostly those with invasive peritoneal implants.
Table 25.3
Death from Tumor among Patients with Ovarian Serous Borderline Tumors Associated with Peritoneal Implants (Literature Review, 1984–2011)14–19,21,31,33,34,42–44
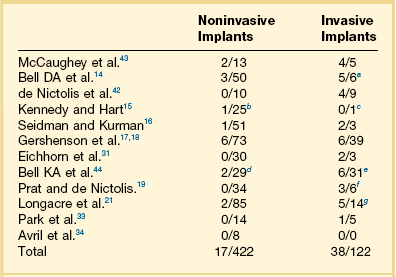
aOne patient died of tumor subsequent to her report.
bTransformation into serous carcinoma.
dOne patient was alive with progressive disease (AWPD).
fThe other three patients were AWPD.
gOne patient was AWPD and one died of leukemia but had persistent tumor.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


