Osteomyelitis occurs because of the virulence of a given organism or its by-products, susceptibility of the host resulting from predisposing insults (trauma, implant insertion), loss of natural barriers (decubitus ulcers, dental procedures), underlying receptive pathophysiology (sickle cell disease), overwhelming of host defense mechanisms (antibiotic resistance, chronic disease), or a combination of these factors (diabetic ulcers). In the preantibiotic era, nearly a fourth of patients with osteomyelitis died.
The clinical and roentgenographic presentation of infections in bone is protean, and the diagnosis should always be considered when a patient presents with abnormal x-ray findings. Although bone infections are most often caused by pyogenic organisms, virtually every organism has been reported to involve bone, including viruses. Bone, with its unique architecture and compartmentalized hypervascular milieu, provides an ideal nidus for the growth of organisms and chronic infection, which further complicates diagnosis and treatment.
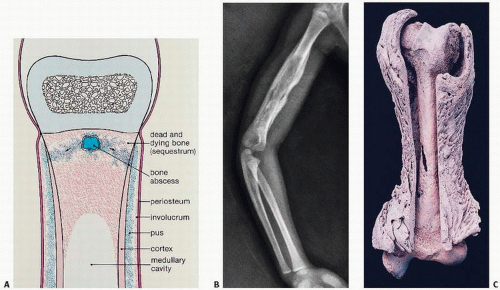
In general, infections of the bone may be considered as acute or chronic. Acute cases generally follow episodes of bacteremia and are characterized clinically by chills, fever, pain, erythema, swelling, tenderness, and usually leukocytosis. Approximately 10 percent of cases of acute osteomyelitis become chronic. Chronic osteomyelitis is more difficult to diagnose, may wax and wane, and eventually destroys bone, resulting in foci of dead bone called sequestra (Fig. 5.1). The marked ability of bone to respond to injury, particularly during growth of the skeleton, may lead to significant formation of new bone. This new bone is referred to as involucrum.
Clinical symptoms of osteomyelitis vary. Adults with hematogenous osteomyelitis usually have vague symptoms: nonspecific pain and low-grade fever of several months’ duration. Tenderness, if present, may not localize to the area of osteomyelitis. Children with hematogenous osteomyelitis may have lethargy, fever, and irritability and may show local signs of infection.
Several systems have been used to classify osteomyelitis (Fig. 5.2) (Table 5.1). A clinically commonly used classification system, known as Cierny-Mader, includes four anatomic stages (Table 5.1) (1). Stage 1 is confined to the medullary cavity as in hematogenous osteomyelitis cases or rod implant infections. Stage 2, or “superficial,” involves only cortical bone and may be due to a contiguous focus or direct inoculation. Stage 3, a localized type, involves cortical and medullary bone, but not the entire bone diameter. Stage 4 is diffuse, involving the entire thickness of the bone. The system further classifies the host according to those with no compromising factors (A) and those with systemic (Bs), local (Bl), or both systemic and local (Bls) compromise. A “C” host defines a patient so severely compromised that treatment may introduce an unacceptable risk.
FIGURE 5.1. Osteomyelitis. A nidus of infection within the bone spreads through medullary (cancellous) and cortical bone and induces periosteal formation of new bone (A). The infected bone eventually becomes dead bone (sequestrum) enveloped by a shell of periosteal new bone (involucrum). Roentgenogram of humerus (B); in a gross femur of a cow (C), note that the entire femur is necrotic, with extensive new periosteal bone enveloping and shaping a new shell contour (involucrum).
The Beit-Cure classification system was developed specifically for chronic hematogenous osteomyelitis in children (2). Three main groups (A, B, and C) are defined: a Brodie abscess type (A), a sclerotic type (C) and a type B, which defines the type of sequestrum and involucrum. This system attempts to define physeal damage and the type of involucrum as it may affect structural support of the bone. A “structural” involucrum is considered one that can provide adequate support for the involved limb to withstand gravity.
In the most common type of osteomyelitis (approximately 50 percent of cases), infection spreads directly from another site. Skin, operative, and posttraumatic infections are the most common sources. It has been estimated that approximately 1 percent of prosthetic joint procedures are complicated by infection. Another large group of osteomyelitis patients (30 percent of cases) have peripheral vascular disease. Here, diabetes is most often the culprit. In diabetes, peripheral vascular disease is further complicated by the development of skin ulcers, which themselves can be foci of infection and therefore a second source of osteomyelitic infection.
Diabetics represent a significant group of patients with osteomyelitis. Foot infections in these patients frequently lead to amputation. In fact, in the majority of diabetic foot ulcers, unsuspected underlying osteomyelitis is present (3). Factors contributing to bone infection in diabetes include both peripheral neuropathy and vascular insufficiency.
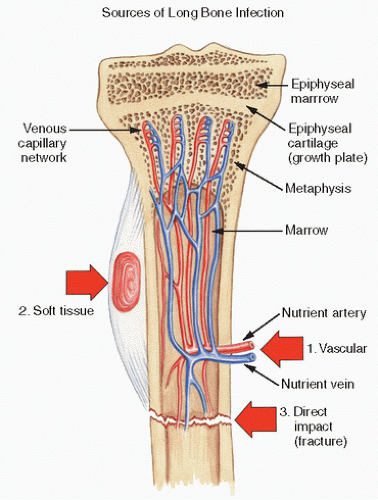
The least common type of osteomyelitis in clinical practice (20 percent of cases) is thought to result from hematogenous spread by bacteria (Table 5.2), often after trauma or medical intervention, such as placement of catheters. In particular, skin, respiratory, and urinary infections predispose to osteomyelitis. Before the advent of antibiotics, hematogenous osteomyelitis led to chronic infection in more than half of patients, with approximately one-fourth dying. Hematogenous osteomyelitis usually begins in the metaphysis of a bone (Fig. 5.1). The metaphysis is thought to be the initial site of infection for anatomic reasons. The branches of the nutrient artery provide an extensive network of vessels to the zones of endochondral ossification in this region (Fig. 5.2). Rather than anastomosing, however, these vessels terminate in venous sinusoids, ideal lakes for bacterial seeding.
These vascular loops and terminal branches have low oxygen tension and inhibited phagocytosis, which is conducive to bacterial growth (4). Assuming theoretical risks such as bacteremia in humans (e.g., dental flossing) and the microtrauma of daily living (bumps on the knee), these anatomically fragile metaphyseal vascular zones take on considerable importance.
Once infection takes hold, it spreads to adjacent trabecular or cancellous bone and eventually laterally to and through the cortex via the haversian canals to the periosteum. The periosteum, initially inflamed, becomes reactive and forms new bone. In addition, the periosteum may actually rupture. Infection in the cortical bone leads to vascular compromise and/or clotting abnormalities, which in turn contribute to bone necrosis.
FIGURE 5.2. Osteomyelitis. Bone infections may be caused by contiguous spread from soft tissue infections; by fractures, especially those involving open wounds; or by hematogenous spread through vascular routes.
Although diaphyseal spread occurs later, the growth plate is a relative barrier to spread, particularly in adolescence, a phenomenon reminiscent of the relative epiphyseal barrier to the spread of osteogenic sarcoma and other bone tumors. This barrier usually prevents contiguous spread to the joint space. The hip and shoulder joints are more prone to involvement, as the synovial attachment occurs lower in the metaphyseal region.
Roentgenographic changes in osteomyelitis appear late and are usually nonspecific (Fig. 5.3) (Table 5.3A).
In hematogenous osteomyelitis, radiographic changes lag at least 2 weeks behind the process of infection. The earliest changes are soft tissue swelling, then focal osteopenia and periosteal thickening or elevation (5). Only new subperiosteal bone growth and the development of a transcortical sinus are reliably specific for infection.
Bone-scanning agents are more sensitive and therefore can be used to confirm the nature of a suspected lesion earlier than can routine x-ray films. However, no nuclear medicine scan is specific for infection (Table 5.3B). A technetium-99m scan may be negative (in 4 to 20 percent of cases) because of decreased blood flow to an osteomyelitis-related focus of osteonecrosis (4). However, technetium scans are sensitive in identifying multiple sites of infection in infants and neonates. Gallium, which attaches to transferrin, leaks in areas of inflammation but, again, is nonspecific for infection-related inflammation and may be positive whenever leukocytes or macrophages aggregate even in tumors.
Gallium-67-citrate-labeled leukocyte scans are positive but expensive, have radiation exposure, and take several days to complete. Indium-labeled leukocyte scans tag neutrophils, but again are nonspecific for that type of inflammation. The sequential use of scans has been used to refine diagnostic acumen, and an infection can be suspected if uptake on gallium or indium is more intense than technetium. However, such costly, radiation-intense, and time-consuming protocols seem hardly appealing.
Computed axial tomography can help in identifying necrotic bone (increased bone density) and soft tissue involvement and ultrasonography in identifying soft tissue swelling.
Additional scanning studies that have been used include 99m Tc-ciprofloxacin (6), technetium-99m-labeled monoclonal anti-NCA-90 antibody to the Fab fragment, and positron emission tomography (PET) scanning (7).
Because leukocyte scanning may lose sensitivity in the leukocyte-rich hematopoietic marrow of the axial skeleton, PET scanning, which exploits the cellular uptake of radiologically traceable glucose, may be better at identifying osteomyelitis in the axial skeleton.
Magnetic resonance imaging (MRI) may be most helpful in defining the extent of infection. In general, osteomyelitis can be suspected when a region of marrow in the clinically suspected site shows a low signal on T1-weighted images and an increased signal on T2-weighted images.
TABLE 5.2 Predisposing Factors for Hematogenous Osteomyelitis
Trauma (more common in men and boys)
Skin, dental, respiratory, gastrointestinal, and urinary tract infections
Bacterial endocarditis
Burns
Leukopenia
Leukocyte dysfunction (e.g., granulomatous disease of childhood)
Complications of pregnancy and delivery
Iatrogenic intervention (e.g., catheters)
Intravenous drug abuse
Sickle cell anemia
Immunosuppressive therapy
Hemodialysis and renal failure
Poor nutrition
Diabetes
Obesity
History of smoking
Hypokalemia
Although bone bruise, trauma, ischemia, and fracture can mimic osteomyelitis on MRI, magnetic resonance imaging gives excellent anatomical information on bone marrow and soft tissue changes (8). Recent developments in imaging osteomyelitis include the use of hybrid PET/MRI scanners, a so-called “one-stop” diagnostic procedure (8). In utilizing PET scans, a cutoff value for the SUV max of 3 has been suggested as giving optimal results (8).
Recently, the use of ultrasound techniques to identify deep soft tissue swelling has been found effective (9,10). However, all clinicians are familiar with the lack of definitive diagnostic accuracy of imaging techniques in osteomyelitis. Because of the protean roentgenographic manifestations of osteomyelitis, the differential diagnosis includes lesions causing periostitis or periosteal formation of new bone, tumors and tumor-like lytic lesions (eosinophilic granuloma, osteoblastoma, osteoid osteoma), permeative lytic tumors (Ewing sarcoma, lymphoma), and ischemic bone syndromes (transient osteoporosis, reflex sympathetic dystrophy). Therefore, it would be prudent to consider osteomyelitis in the differential diagnosis of all orthopaedic and joint presentations with ambiguous clinical and roentgenographic findings.
A summary of imaging procedures used in the diagnosis of osteomyelitis is given in Figure 5.3B.
Hematogenous Acute and Subacute Pediatric Osteomyelitis
It has been estimated that acute osteomyelitis occurs in about 8 in 100,000 children per year in high-income countries. Delay in diagnosis of acute pediatric osteomyelitis can result in devastating complications, including sepsis, chronic infection, disruption of longitudinal growth, angular bone deformities, and high morbidity (10,11). Forty percent of children are afebrile with the following distribution of skeletal involvement:
Site
Incidence (%)
Femur
26.9
Tibia
26.0
Pelvis
9.2
Humerus
8.1
Foot
7.7
Forearm
4.8
Calcaneum
4.6
Vertebra
3.8
Fibula
3.7
Hand
2.0
Clavicle
0.8
Rib
0.6
Patella
0.2
Other
1.6
Most children have localized signs and symptoms including pain. About half have a reduced range of motion and reduced weight-bearing, limping or inability to walk. Staphylococcus aureus is the most common causative organism followed by the respiratory pathogens Streptococcus pyogenes and S. pneumoniae. While Kingella kingae infections are increasing and most often found in children under 4 years of age, Haemophilus influenzae type b is more likely to affect joints rather than bones.
Many factors contribute to the development of osteomyelitis, including host defense (e.g., status of inflammatory response), characteristics of the bacteria (e.g., endotoxin formation), and bacterial processes (e.g., biofilm formation). Within the host, neutrophils play a significant role and are a distinguishing feature in the light microscopic diagnosis in osteomyelitis. In fact, osteomyelitis is common in acquired neutropenias (e.g., chemotherapy) and leukocyte dysfunction syndromes, such as chronic granulomatous disease of childhood. Less important is cell (T cell)-mediated immunity, osteomyelitis being rare in the acquired immunodeficiency syndrome (AIDS).
The integrity of endothelial cell lining is important in that it may cover up underlying adhesion receptors on collagen and fibronectin; these receptors play a role in forming ligands for bacterial adherence. Possible ligands for such bacterial connections include collagen receptors in cartilage (12) and, in bone, proline-rich proteins of the collagen organic matrix of normal bone, bone sialoprotein, and exposed collagen protein in traumatized bone.
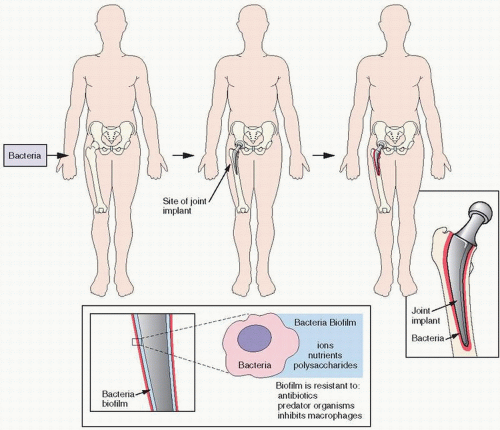
A significant event in osteomyelitis associated with implant devices appears to be the development of a biofilm that coats the bacteria, which may inhibit macrophages and enhance resistance, not only to predator organisms but also to antibiotics. Biofilms are complex and probably consist of ions, nutrients, and polysaccharides (Fig. 5.4) (see Chapter 17).
The most important cell in fighting infection is the neutrophil (polymorphonuclear leukocyte). Both congenital and acquired neutrophil problems predispose to osteomyelitis. Causes of acquired problems are numerous and include cytotoxic chemotherapy, anti-inflammatory agents (such as steroids), and factors that interfere with leukocyte migration (such as vascular disease and radiation). Normally, polymorphonuclear leukocytes phagocytize bacteria that have been opsonized through potent adhesins, such as fibronectin or laminin. Opsonized bacteria link to receptors on polymorphonuclear leukocytes, which lead to phagosome formation, cytoplasmic invagination, and phagolysosome-mediated destruction. In addition, substances such as lysozyme, a leukocyte enzyme, lyse gram-negative bacteria. In fact, the body normally contains a wide array of substances that fight bacterial infections (13). These include serum substances such as properdin, complement, β-lysins, and immunoconglutinins. Complement is key to numerous bactericidal functions.
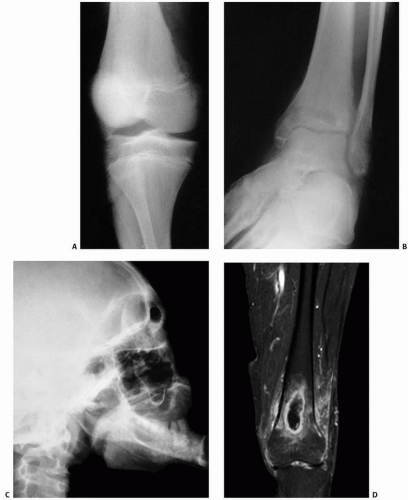
FIGURE 5.3. Osteomyelitis. Roentgenographic changes include lucency (A), mixed lucency and sclerosis (B), and marked sclerosis (C). In (A), an area of lucency is seen in the cortex of the metaphysis of the distal femur. In (B), a poorly defined lucent region of the distal end of the tibia is noted; periosteal reactions medially and laterally indicate the acute nature of infection. In (C), a poorly defined area of sclerosis is seen in the body of the mandible. A Gd-enhanced T1-weighted spectral fat-saturated MRI image shows a sharply demarcated lesion with fluid content and ring enhancement. Also note the enhanced bone marrow and soft tissue edema (D). Osteomyelitis in the third finger (Continued)
FIGURE 5.3. (Continued) (E). Radiograph of the hand showing mixed lucent and sclerotic destruction in the proximal phalanx of the third digit (F). Coronal T2 MRI showing low signal in center of lesion and extensive soft tissue change (G). OR photograph (H). (Figure D reprinted with permission from Demirev A, Weijers R, Geurts J, et al. Comparison of (18F) FDG PET/CT and MRI in the diagnosis of active osteomyelitis. Skeletal Radiol. 2014;43:665-672.)
TABLE 5.3A Roentgenographic Changes in Osteomyelitis
>24 h
→
Positive bone scan
>3 d
→
MRI shows deep soft tissue swelling
3-10 d
→
MRI shows muscular edema and obliteration of fat planes
10-14 d
→
Osseous changes including demineralization
3-6 wk
→
Periosteal new bone formation Sequestra Involucrum
h = hours, d = days, wk = weeks
TABLE 5.3B Imaging for Osteomyelitis
Sensitivity
Specificity
Positive Predictive Value
Advantages
Notes
Radiography
16%-20%
80%-100%
96%
Cheap, easily obtainable, and safe way of monitoring disease progression.
Abnormal admission x-rays (not soft tissue swelling) seen less often in acute osteomyelitis (bone destruction, lytic lesions, and periosteal reaction)
Tc-99 bone scan
53%-100%
50%-100%
39%-82%
No anesthetic, widely available, good for localizing lesion(s). Indicates vascularity and/or new bone formation.
5%-18% positive scans are cold, and patients need aggressive treatment
MRI
80%-100%
70%-100%
84%-93%
No radiation. Identifies local complications: abscess or joint/physeal involvement.
Bright T2 signal indicates edema and inflammation
PET/CT
92%
92%
Can differentiate between degenerative and infective changes.
Good for screening for unknown fever
CT
67%
50%
65%
Best at demonstrating cortical destruction, periosteal reaction, bone gas, and sequestrum, but these are often absent until later stages.
Reserved for when other investigations are not possible or inconclusive
Ultrasound scan
55%
47%
82%
Shows soft tissue swelling. Reliable, cheap, quick, nonionizing, and easily obtainable. Good aid in deciding if surgery is required and in differentiating between osteomyelitis and soft tissue abscesses, cellulitis, and pyomyositis.
If treated nonsurgically, repeated ultrasound scans are useful to monitor abscess resolution or progression. Improvement on ultrasound and falling C-reactive protein (CRP) correlates well with clinical findings. Sensitivity and specificity are high for detecting complications (74% and 85%, respectively)
Modified from Dartnell J, Ramachandran M, Katchburian M. Instructional review: children’s orthopaedics. haematogenous acute and subacute paediatric osteomyelitis. A systematic review of the literature. J Bone Joint Surg Br. 2012;94:584-595.
Some common measured laboratory serum analytes may also indicate infection. C-reactive protein (CRP) has been demonstrated to enhance bacterial phagocytosis (14,15), and transferrin may enhance bacterial resistance by denying needed iron.
However, bacteria have numerous mechanisms to elude neutrophil-mediated destruction. One such mechanism is the formation of a biofilm. Most potent, however, is the production of endotoxin, the lipopolysaccharide coat that characterizes gram-negative bacteria. The mechanism of endotoxin production in sepsis is via complement, which activates numerous cells, including polymorphonuclear leukocytes and monocytes. Through subsequent tissue events (e.g., vascular response), cell events (e.g., the production of proteases, arachidonic acid metabolites, and toxic oxygen metabolites), and cell-to-cell messages facilitated by cytokines (interleukins and tissue necrosis factor) and platelet-activating factor, a vicious, self-perpetuating cycle ensues and results in tissue destruction and hypotensive organ failure.
FIGURE 5.4. Osteomyelitis. Implants may be covered by a biofilm consisting of a slimy composite of ions, nutrients, and other substances. The biofilm provides fertile territory for bacteria, and resistance to macrophages, antibiotics, and predator organisms.
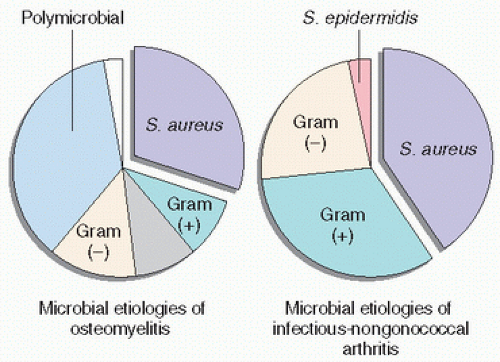
The most common causative agent of osteomyelitis is S. aureus, followed distantly by Staphylococcus epidermidis, gram-negative organisms, anaerobes, and others (16) (Fig. 5.5) (Table 5.4).
In infants, the most common isolates are S. aureus, Streptococcus agalactiae, and Escherichia coli. In children older than 1 year, S. aureus, S. pyogenes, and H. influenzae are most common. H. influenzae, which decreases after age 4 years, has been shown to have an overall decreasing incidence in recent years, a phenomenon that has been attributed to the new H. influenzae type B vaccine.
Gram stain differentiates bacteria based on the ability of some of them to counterstain (usually with safranin O) after the initial crystal violet stain has been rinsed. Gram-positive organisms remain dark (purple), whereas gram-negative organisms appear pale or pink (13). Table 5.5 lists the bacteria according to staining and anaerobic/aerobic status.
In general, S. aureus is the most common agent in hematogenous osteomyelitis and osteomyelitis, resulting from a contiguous focus of infection and vascular insufficiency. It is the most common agent in osteomyelitis in patients of all ages. Gram-negative bacilli and anaerobes predominate in patients with decubitus ulcers. Other interesting associations are noted in Table 5.6.
FIGURE 5.5. Osteomyelitis. Microbial etiologies.
TABLE 5.4 Bacteriology of Osteomyelitis
Acute Osteomyelitis
Chronic Osteomyelitis
Staphylococcus aureus
S. aureus
Streptococci
Gram-negative bacilli
Gram-negative bacilli
Streptococci
Sterile
Staphylococcus epidermidis
S. epidermidis
Sterile
Haemophilus influenzae
Anaerobes
Anaerobes
H. influenzae
From Wheat J. Diagnostic strategies in osteomyelitis. Am J Med. 1985;78:218-224.
Whereas the incidence of hematogenous osteomyelitis appears to be on the decline, osteomyelitis due to contiguous foci of infection or direct inoculation is on the rise and in part attributable to the use of orthopaedic devices.
S. Aureus
Staphylococcus aureus (Staph aureus) can cause as broad an array of clinical infections as any known microorganism. From chronic skin infections to fatal sepsis, it can infect virtually any tissue.
Why is S. aureus such a common isolate in bone and periprosthetic infection? After all, humans are a natural reservoir of this bacterium, with many people having “normal” colonization in nares, armpits, pharynx, and skin (17). For one, S. aureus contains or accrues adhesion molecules that facilitate its binding to bone matrix. This includes, most notably, fibronectin-binding protein. In addition, staphylococci can secrete toxins capable of bone resorption and have also been shown to be internalized by osteoblasts and osteocytes (18). The demonstration that bacteria can be sequestered from the host immune system may be critical in understanding reactivation of infection, long a poorly understood phenomenon (19).
Elements that facilitate staphylococci infectivity and potency include the following:
Peptidoglycans that may have endotoxin-like activity stimulating the release of cytokines by macrophages and activation of complement
Antiphagocytic polysaccharide capsules, which may also add to the virulence of methicillin-resistant S. aureus (MRSA), a growing infectious troublemaker
Cell wall-binding proteins and ligands, some of which can bind extracellular matrix molecules such as those of dead bone, grafts, and implants
Cytotoxins such as those causing toxic shock syndrome
Destructive enzymes such as proteases, coagulases, lipases, and hyaluronidases
MRSA has emerged as a problematic pathogen with estimates that infections by MRSA in orthopaedic wards can double the mortality rate with infection correlating with increased length of hospital stay (20).
Community-acquired MRSA strains often share staphylococcal cassette chromosome mec (SEC mec) type IV that contains the gene responsible for methicillin resistance. MRSA also contains the genes for Panton-Valentine leukocidin (PVL) toxin. When released, the PVL toxin degrades white blood cells, resulting in an extremely virulent strain of the bacterium while nasal colonization of Staph aureus is about 30 percent. Colonization by MRSA is 1 to 2 percent.
Special Clinical Associations
Specific clinical associations are listed in Tables 5.6, 5.7 and 5.8. Diabetics, in addition to S. aureus, often grow enterococcus, Group B Streptococcus, Peptococcus, Klebsiella, and Proteus mirabilis. Peripheral vascular disease, peripheral neuropathies, osteopenia, diminished immune and healing capabilities, and poor compliance complicate the diabetic picture.
Pharyngitis and dental plaques often grow Fusobacterium necrophorum, a spindle-shaped, gram-negative anaerobic bacillus that has been associated with septic arthritis of the knee.
Salmonella enterica, which is abundantly present in the stool of infected persons, can contaminate water and food, and shows a remarkable ability to survive intracellularly.
The fungi that may harbor in a natural joint include Coccidioides, Blastomyces, and Sporothrix species, with Candida more likely in an implant joint.
Dental procedures have been reported to precede late periprosthetic infections in 6 percent of cases with Streptococcus viridans and Peptostreptococcus as isolates (21).
Infected dog and cat bites may lead to Pasteurella infections as well as anaerobes such as Fusobacterium and Bacteroides (22).
TABLE 5.5 Gram Staina: Gram-Positive Versus Gram-Negative Bacteria
Purple (Dark) Staining (Gram-Positive)
Pink Staining (Gram-Negative)
Pathologic features
Cytoplasmic membrane and cell wall components that may enhance virulence
Outer membrane lipopolysaccharide (endotoxin) that provides virulence
Possess pili that allow attachment to epithelial cells
Examples
Staphylococcus aureus
Enterobacteriaceae
Staphylococcus epidermidis
Escherichia
Enterococci
Klebsiella
Aerobic and anaerobic streptococci
Proteus
Enterobacter
Serratia
Clostridium
Citrobacter
Bacillus
Edwardsiella
Diphtheroids
Erwinia
Listeria
Aeromonas
Salmonella
Shigella
Gram-negative rods
Pseudomonadineae
Haemophilus influenza
Brucella
Campylobacter
Bordetella
Yersinia
Pasteurella
Francisella
Aerobic gram-negative cocci
Neisseria
Branhamella (dentally/orally related)
Moraxella
Acinetobacter
Anaerobic gram-negative rods
Bacteroides
Fusobacterium
Eikenella (aerobic)
aCrystal violet-iodine complex, rinsed with alcohol, counterstained with contrasting dye (safranin O). Modified from Merritt K. Gram-negative microorganisms and microbial adhesion. In: Esterhai JL, et al., eds. Musculoskeletal Infection. Park Ridge, IL: American Academy of Orthopaedic Surgeons; 1992:79-88.
TABLE 5.6 Bacterial Associations in Specific Clinical Situations
TABLE 5.7 Anaerobic Osteomyelitis and Arthritis (in Order of Frequency)
Bone
Joints
Bacteroides
Propionibacterium acnes
Anaerobic cocci (streptococci)
Anaerobic cocci
Fusobacterium
Bacteroides
P. acnes
Clostridium
Clostridium
Reprinted from Brook I, Frazier EH. Anaerobic osteomyelitis and arthritis in a military hospital; a 10-year experience. Am J Med. 1993;94:21-28, with permission.
Necrotizing Fasciitis
Necrotizing fasciitis is a rapidly progressive life-threatening soft tissue infection. It involves the superficial fascia and subcutaneous tissue and has been categorized as follows:
Type I, a mixed infection with aerobic and anaerobic bacteria,
Type II, group A β-hemolytic streptococcus or S. aureus,
Type III, a marine vibrio, a species endemic to warm coastal waters and raw seafood.
Necrotizing fasciitis is a surgical emergency requiring early diagnosis, surgical debridement, and broad-spectrum antibiotic therapy.
Diagnosing Osteomyelitis
There is no single laboratory or radiologic test that can unequivocally diagnose osteomyelitis. Short of grossly observable pus, the clinician is dependent on a range of tests to help establish the diagnosis (Table 5.9).
White Blood Cell Count
The white blood cell count may be normal in osteomyelitis, and when positive, is a nonspecific finding. The white count may be especially misleading in neonates, who, having an immature immune system, are less able to produce an inflammatory response. Add to this the fact that 30 to 40 percent of cases of subacute osteomyelitis have had previous trials of antibiotics; the white cell count, differential, and even cultures can be misleading.
TABLE 5.8 Clinical Correlations in Anaerobic Bone and Joint Infections
Pigmented Prevotella and Porphyromonas, Fusobacterium
Vascular disease
Bacteroides fragilis Neuropathies
Joints
General
Trauma, prior surgery, presence of prosthetic joint, contiguous infection
Prosthetic joints
Propionibacterium acnes
Hematogenous spread
B. fragilis
Lower extremity compound fractures
Clostridium
TABLE 5.9 Studies for the Detection of Musculoskeletal Infection
Serologic
Histologic
Radiographic and Scintographic
Culture
Molecular
White blood cell count
Gram stain Intraoperative frozen section
Plain radiographs Ultrasound, MRI
Aspiration and culture Intraoperative culture
Polymerase chain reaction (PCR)
Erythrocyte sedimentation rate
Triple-phase bone scan
Reverse transcriptase PCR
C-reactive protein
Indium-labeled white blood cell count scan
Ligase chain reaction
Interleukin 6
[18F]FDG/PET scan
Branched chain reaction
Pro-calcitonin
Restriction fragment length polymorphisms
Synovial fluid
Enzyme-linked immunoassays
Leukocyte esterase test
Chemiluminescent oligonucleotide probe
α-Defensin test
Modified from Hoeffel DP, Hinrichs SH, Garvein KL. Molecular diagnostics for the detection of musculoskeletal infection. Clin Orthop Rel Res. 1991;360:37-46.
Erythrocyte Sedimentation Rate and C-Reactive Protein
It is unlikely that a patient has osteomyelitis if both the erythrocyte sedimentation rate (ESR) and CRP are negative. The ESR is a manifestation of enhanced red blood cell aggregation. Red blood cells normally have a negative charge that keeps them repelled from one another. With inflammation and coating with fibrinogen and other substances, red blood cells aggregate. CRP (normal 0.3 to 1.7 mg/L) is an acute phase response protein produced in hepatocytes by cytokine stimulation (especially interleukin 6 [IL-6]). CRP derives its name from the discovery that serum from ill patients precipitates the C-polysaccharide of the cell wall of pneumococci. Its half-life is about 6 hours, and it peaks 48 hours after stimulation. CRP rises faster and returns to normal more quickly than the ESR. CRP peaks at 2 days and returns to normal after treatment. Sustained elevation suggests ongoing infection or inflammation. CRP is usually measured in clinical laboratories by either immunonephelometric or immunoturbidimetric assays, which have a limit of detection of 0.3 to 0.5 mg/dL (23). It peaks at about 8 hours after a stimulus.
IL-6 has recently been investigated for its use in diagnosing periprosthetic infection and correlates well with CRP. CRP and IL-6 provide a better positive predictive value and negative predictive value for the diagnosis of sepsis than either marker alone.
Additional laboratory markers to identify infection include the identification of exocellular glycolipid antigens (24), serum IgG to exocellular bacterial antigen (including lipids), decreased lactic acid as a negative marker, increased acidity, and neutrophil gene expressions.
Synovial fluid biochemistry is significantly altered in infected joints with pH levels usually below 7.2, pCO2/pO2 ratios above 2.5, and glucose levels below 2.5 mmol/L.
Gram Stain
There are vagaries associated with the performance of Gram stains, which limit their use and value in diagnosing infection when not performed by laboratory experts. There may be under- or overdecolorization, smear thickness may interfere with interpretation, and because at least 10,000 bacteria/mL are required to be seen, smears can be falsely negative. Fibrin may interfere with the interpretation of gram-negative stains (red) and white cell debris and microcalcifications with gram-positive stains (black).
Cultures
Cultures have been reported to be falsely negative in up to 40 percent of cases of infection. Some causes of false negativity include low-grade infections, infections with low-grade bacteremia (<1 organism/mL), intermittent bacteremia, loculated infections such as small abscesses, and sterilization by preculture antimicrobial therapy. In addition, collection problems may interfere with accuracy such as with inappropriately collected, stored, or transported specimens. Delay in transport to the laboratory is an especially important factor for culturing anaerobes.
Swabs are not as effective as sampling tissue, especially for fungal organisms and tuberculosis (TB). A mini-swab has a 1,000 times less specimen than a container with 15 mL of fluid or tissue, that is, a 1,000 times less chance of recovering an organism. Swabs, in general, are notoriously inadequate for identifying mycobacteria and fungi. Although colonization by bacteria is not uncommon on surfaces and membranes, clinically significant bacterial infection usually occurs in tissue and confined anatomical spaces. To improve the quality of cultures, one should sample and culture curetted bone, the bed of involved bone, sinus tracts, and the purulent tissue if identified.
In general, extrapolating from the bone allograft literature:
Single cultures do not identify all bacteria that are potentially present and important.
Cultures are frequently positive for low quantities of common skin commensals (e.g., coagulase-negative staphylococci).
A negative culture does not preclude the presence of osteomyelitis.
There is no established cutoff number of culture-positive specimens that warrants corrective action (25).
Organisms identified by a swab of a wound or needle biopsy may not be representative of the pathogens present (26).
The absence of growth of an organism does not rule out the possibility of reactivation and better detection after a surgical procedure.
As for false positivity in cultures, a new body of literature suggests conventional thinking about the meaning of a positive culture warrants reassessment (27). In some studies, culture-positive cases have had little effect on femoral head bone graft outcomes at the 1-year mark (28).
Molecular Diagnostics
Numerous molecular diagnostic techniques have been introduced to provide more rapid results and to help identify bacteria that are difficult to isolate due to current antibiotic use, fastidious organisms that are difficult to grow, and organisms causing low-grade infections. Techniques are focused on identifying the 16S rRNA factor unique to prokaryotic bacteria, that is, bacteria of importance for human illness. These techniques rely either on amplification of bacterial component (e.g., polymerase chain reaction [PCR]) or on nonamplification techniques.
Although many of these techniques are gaining widespread application in detecting Mycobacterium tuberculosis, Treponema pallidum (syphilis), Bordetella pertussis, and Neisseria gonorrhoeae, the major limiting factor in more widespread application is the remarkable sensitivity at the expense of specificity. That is to say, clinically insignificant low bacterial colony counts, fragments of dead bacteria, possible laboratory contaminants, or clinically irrelevant isolates may lead to false positives and the identification of really meaningful bacterial growth (29).
Conversely, bacteria engulfed in biofilm may lead to a false-negative result.
Histology
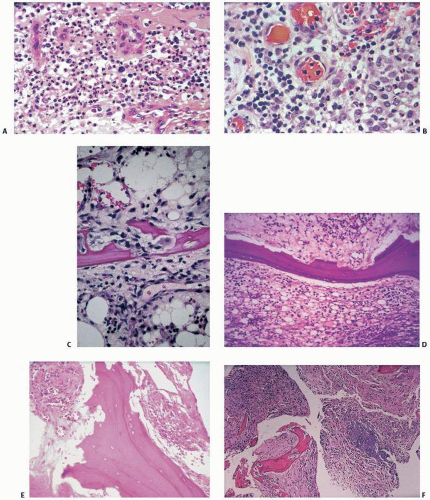
The characteristic histopathologic findings in acute osteomyelitis are the following (Fig. 5.6):
Polymorphonuclear leukocytes
Intravascular polymorphonuclear leukocytes
Osteoclastic bone resorption
“Bitten” bone (chewed, scalloped bone)
Bone necrosis
“Dirty marrow”
“Creeping substitution,” that is, the juxtaposition of new bone on old or dead bone
Vessel damage
Vascular thrombosis
Marrow infarction
Biofilm formation
And in chronic osteomyelitis:
Accumulation of plasma cells and mononuclear cells
Marrow fibrosis
Creeping substitution
If joint cartilage is involved, chondrolysis occurs. Chondrolysis is characterized by polys tracking into cartilage, staining pallor, and empty and expanding chondrocyte lacunar spaces.
The histology of osteomyelitis follows a predictable temporal sequence. Initially, within 24 to 48 hours, polys are recruited to the site of infection, and there is limited vessel wall alteration and limited thrombosis. Inflammation is confined to the medullary canal, but eventually tracks through the bone seeking “escape,” which, if through the cortex, creates a “cloaca” or opening. There are eventual osteonecrosis, hordes of inflammatory cells, and bone resorption (evident on x-ray examinations at about 8 to 12 days). Osteonecrosis occurs and, if the necrotic area is small, a cavity is left behind. Large zones of osteonecrosis (“the sequestrum”) create a milieu for bacterial concentration and growth. Infection and inflammation spread to and through cortical bone, elevating the periosteum, leading to an encasing sheath of new bone called the “involucrum.” Periosteal elevation is most pronounced in children who have a looser fibrous periosteum. In adults, tracking through the cortex and periosteum may lead to sinus formation.
Polys, local vascular proliferation, local edema, and necrotic bone set in place a vicious cycle with diapedesing polys altering the wall of local vessels, leading to vascular congestion and thrombosis, itself leading to decreased flow, local pressure buildup, further thrombosis, and further bone necrosis. The adhesion of polys to the endothelial wall activates a plethora of local tissue factors:
Tumor necrosis factor
Interleukin 1, 6, 8, and 10
Oxygen radicals
Platelet-activating factor
Proteases
Prostaglandins
Leukotrienes
Bradykinin
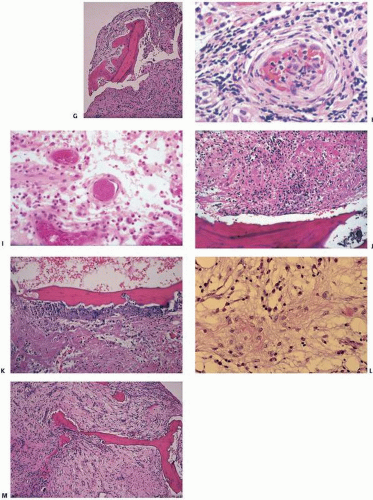
FIGURE 5.6. Osteomyelitis at a glance. (A) Polymorphonuclear leukocytes. (B) Intravascular polymorphonuclear leukocytes. (C) Osteoclastic bone resorption. (D) “Bitten bone” (chewed or scalloped). (E) Bone necrosis. (F) “Dirty” marrow. (Continued)
FIGURE 5.6. (Continued) (G) Creeping substitution, which is the juxtaposition of new bone on old bone. (H) Vascular damage, that is, endothelial cell proliferation and hyperplasia. (I) Microthrombi. (J) Marrow infarction, that is, loss of background architectural detail. (K) Biofilm formation. (L) Plasma cells and mononuclear cells. (M) Marrow fibrosis.
Many of these cause further damage, promoting microthrombosis. In addition, a biofilm-like slime coats necrotic bone surfaces, and along with necrosis of bone and local tissues, promotes in vivo bacterial adherence and growth.
In addition to bacterial protection in the glycocalyx slime of biofilm, they can elude host defenses by gaining access to cells including osteoblasts. Recent evidence of osteoblasts and osteocytes harboring S. aureus gives credible scientific support to the recrudescence, reactivation, and flare-ups of osteomyelitis.
Anaerobic Osteomyelitis
More than 1,000 cases of anaerobic osteomyelitis and arthritis have been reported in the literature. Bacteroides species and anaerobic streptococci are the most common organisms at all sites (30,31) (Table 5.7). Clinically, in anaerobic osteomyelitis, more than 90 percent of patients have fever, pain, and leukocytosis. The white blood cell count is greater than 10,000/mm3, with an observed malodorous pus in about half of patients. An elevated ESR is observed in three-fourths. Bone scans in one series were positive in only 21 percent (30). Patients with anaerobic septic arthritis were symptomatic for a mean of 4.5 days (range, 1 to 23 days) and had fever (80 percent), leukocytosis (74 percent), and an elevated ESR (70 percent). More common symptoms were pain and swelling of the joint (95 percent).
Noteworthy clinical correlations in anaerobic infections are listed in Table 5.8.
Osseous actinomycosis is a rare and usually chronic, indolent disease that can mimic malignancy. Although imaging findings are nonspecific, presentations suggesting the diagnosis include mass-like spread across tissue planes, sinus tracts that spontaneously resolve and recur, and relapse after antibiotic therapy.
The organisms are filamentous, branching, gram-positive, pleomorphic, non-spore-forming, non-acid-fast anaerobic bacteria. Microscopically one can identify granulation tissue and purulent loculations with neutrophils, often appearing as small, hard, pale yellow “granules” (so-called sulfur granules) (32). Often difficult to identify in routine hematoxylin and eosin staining, special stains such as Gomori methenamine silver (GMS), periodic acid-Schiff (PAS), and Brown-Benn stains can be helpful. These organisms typically invade directly from soft tissue, in particular in the vicinity of the jaw (mandible more often than maxilla) after fracture, tooth extraction, or periodontal or sinus infection. Hematogenous spread is rare, and thus results of blood cultures are negative. Actinomyces can be recovered from the joint in infected cases.
Leprosy (Hansen Disease)
It has been estimated that there are 4 million individuals disabled by leprosy worldwide, with 750,000 new cases diagnosed each year (33). Characterized by skin lesions and peripheral nerve damage, the pathology is that of destruction of Schwann cells and axons by CD4+ T-cell-mediated granulomatous inflammation. Osteoarticular manifestations are the result of impaired nerve function with resultant anesthesias, ulcerations of skin, and osteomyelitis. In addition, muscle imbalance, excess trauma, and deformities can ensue. Direct extension of infection to the bone can cause periostitis and subsequent osteomyelitis.
Mycobacterium leprae are demonstrable in tissue section as acid-fast rods with rounded ends.
Leprosy is spread not by touching but by entering the human body through the upper respiratory tract.
In infection with M. leprae, clinical pathologic syndromes may develop that are characterized by abundant proliferation of organisms in tissue histiocytes (lepromatous leprosy) or epithelioid granulomatous inflammation (tuberculoid leprosy). M. leprae is an acid-fast rod that grows best in cool tissues such as the skin, nerves, upper respiratory tract, testes, and anterior chamber of the eye.
The histiocytic proliferation of the lepromatous type leads to cystic destruction of bones and slowly progressive osteomyelitis at the ends of bones. Because spread is contiguous from skin and mucosal lesions, the skull and hands are most frequently affected. In tuberculoid leprosy, peripheral nerves are involved, leading to severe neuropathic changes that compound the direct, bacterially induced, inflammatory destruction. Periostitis, thinning and even total resorption of bones (especially hands and feet, so-called licked candy stick), and neuropathic changes in the wrist and ankle are well described and include tarsal disintegration, paralytic deformities of the metatarsophalangeal joints, clawed toes, and drop foot. Specific bone destruction can lead to rarefaction of the face, hands, and feet.
Researchers remain hampered by M. leprae’s refusal to grow in cell culture or nearly any nonhuman animal.
Armadillos are now a reservoir for the disease and, in coastal marsh habitats where population densities of the animal can be high, 20 percent or more of the armadillos are thought to be infected with M. leprae and capable of passing it on to susceptible people. Of the 200 cases of leprosy diagnosed annually in the United States, most are thought to stem from contact with armadillos, although the precise route of transmission remains unclear.
Syphilis
In the past decade, syphilis, caused by the bacterium T. pallidum, has been increasingly reported in both rural and urban areas of the United States (34). Its increase has been associated with illegal drug use and concomitant prostitution activities, AIDS, and limited access to health care. Although clinical staging is important, primary syphilis denotes the skin lesions or chancres that typically develop about 3 weeks after exposure, and secondary syphilis shows the hematogenous dissemination of T. pallidum and the associated manifestations—“the great masquerader” (31) (Fig. 5.7). Syphilis is seen histologically as a plasma cell inflammation. Spirochetes can be seen microscopically. After latency, syphilis appears with histologically defined gummas—chronic inflammatory destructive lesions that can burrow through cortical bone to leave holes, the markers by which anthropologists identify syphilis in bone. Spirochetes, frequent in acute syphilis, are rare in gummas, which consist of chronic inflammatory cells, macrophages, fibroblasts, and areas of necrosis.
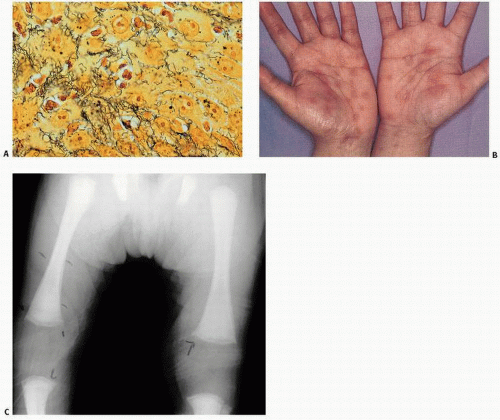
FIGURE 5.7. Syphilis. (A) Spirochetes appear as fine, threadlike corkscrew organisms infiltrating infected tissue (silver stain). (B) Classic features of syphilis include symmetric, dusky red rashes on the palms of the hands and soles of the feet. (C) Roentgenographic features include periosteal reactions along the shafts of the femora and small erosions at the edge of femoral and tibial metaphyses (Weinberger sign). (Modified after Potts SR. Images in clinical medicine. N Engl J Med. 1993;329:176-180.)
Congenital syphilitic osteomyelitis is characterized by nonspecific changes of the bone, including periostitis and inflammation of the zones of endochondral ossification of the growth plates of long bones and less frequently of the vertebrae, flat bones, and short tubular bones (35,36). The widened and irregular growth plates may mimic rickets. Adult acquired syphilis is characterized by perivascular inflammation and periostitis, often with necrotizing inflammatory burrowing through the cortical bones of, in particular, the skull and palate. Periostitis leads to unusual remodeling of the tibiae (“saber shins”).
The laboratory diagnosis of syphilis usually involves serology screening with the Venereal Disease Research Laboratory (VDRL) titer test or other tests such as a microhemagglutination assay for antibodies against Treponema pallidum.
Granulomatous Infection of Bone and Joints
Granulomas are organized inflammatory reactions, and the differential diagnosis is broad. Excluding foreign bodies, the differential diagnosis of granulomatous disease in bone and joints includes sarcoidosis, TB (mycobacterial, atypical), histoplasmosis, coccidioidomycosis, blastomycosis, sporotrichosis, and salmonellosis.
Sarcoidosis
Sarcoidosis is a systemic granulomatous disease of unknown etiology, but it most likely represents a dysfunctional immune system with an estimated prevalence of 10 to 20 per 100,000 (37). Skeletal involvement is rare, most often affecting small bones of the hands and feet. The disorder may be self-limited or chronic. Three major events are necessary for disease expression: (a) exposure to antigen, (b) acquired cellular immunity against the antigen mediated through antigen-presenting cells and antigen-specific T lymphocytes, and (c) the appearance of immune effector cells that promote a more nonspecific inflammatory response. More common in women and in blacks, it is usually diagnosed in young adults. Patients may be asymptomatic, or the disease may be discovered incidentally on routine films of the chest by the presence of mediastinal or hilar lymphadenopathy. However, the array of clinical findings in patients with sarcoidosis is broad, ranging from eye, salivary gland, pulmonary, skin, and nasal lesions to hepatosplenomegaly. The laboratory findings may include mild to moderate elevations of the ESR, lymphopenia, reversal of the albumin-globulin ratio, and abnormal results of liver function tests. However, the disorder is most often characterized pathologically by hypercalcemia, elevated serum levels of angiotensin-converting enzyme (ACE), and the presence of granulomas in tissue sections (Fig. 5.8).
Broadly speaking, sarcoidosis may be differentiated into an acute and a chronic form. The acute form has a sudden onset, usually before the age of 30 years, and is characterized by bilateral hilar lymphadenopathy, acute iritis, conjunctivitis, erythema nodosum and vesicles or maculopapular rashes of the skin, a transient periarthritis, and splenomegaly. There may be bone cysts. Granulomas are typical in tissue sections, with hypercalcemia, hypercalciuria, and high serum levels of ACE. There is usually a frequent spontaneous remission with a good prognosis.
The chronic or persistent form of sarcoidosis, with an onset that is usually insidious, tends to occur in older people. It is characterized by eventual pulmonary infiltration and fibrosis, keratoconjunctivitis, chronic uveitis, and plaquelike skin scars and keloids. Bone cysts may be present; they do not appear in the acute type. There may also be nephrocalcinosis and, often, permanent periarthritis, lymphadenopathy, and splenomegaly. In the chronic type, serum levels of ACE and lysozyme may not be raised. Spontaneous remission of the disorder is rare; recurrence is frequent after steroid therapy, and the prognosis is poor.
As mentioned, classic sarcoidosis is characterized pathologically by elevated serum levels of ACE, hypercalcemia, and granulomas in tissue sections. Elevated serum levels of ACE and calcium are most likely the result of the peculiar granulomatous reaction in sarcoidosis. Historically, the combined Kveim test was used to diagnose this disorder. The Kveim test consists of intradermal injection of a heat-sterilized suspension of sarcoid tissue, usually spleen or lymph nodes. Results are positive in about 80 percent of patients with sarcoid. Histologic examination of the test site is required 6 to 8 weeks after the injection, with the test site tissue revealing well-defined epithelioid cell granulomas similar to those seen in clinical sarcoid. This test is rarely performed clinically today. However, the identification of granulomas in tissue sections and the exclusion of all other causes of granulomas may establish, in the appropriate clinical setting, the diagnosis of sarcoidosis.
Granulomas, by definition, are organized inflammatory reactions with a predictable architectural arrangement. They consist of mononuclear cells, including mononuclear phagocytes and multinucleated giant cells. Immune markers have revealed the presence of T lymphocytes and B lymphocytes as well as fibroblasts. In fact, the granulomas of sarcoid have been extensively studied, and reveal a complex array of phagocytic and lymphoid cells (Fig. 5.8). As mentioned, granulomas occur in a wide range of disorders that include infectious diseases such as TB and fungal infections as well as conditions caused by exposure to inert substances.
In sarcoidosis, the noncaseating granulomas are usually discrete, organized arrangements of mononuclear and epithelioid (i.e., mimicking epithelial) cells and giant cells with abundant fibroblasts. Immunologic studies have identified activated macrophages positive for HLA-DR; these are most likely the first cells activated by the as yet unidentified antigen, which may itself trigger the development of immune complexes. Cell-surface gene products on various cells in sarcoid-predisposed persons lead, through the interaction of glycoprotein lymphokines or T-cell activators, to the production of T-lymphocyte helper cells. Further lymphokine activity may lead to the production of B cells and the eventual production of immunoglobulin and even autoantibodies. The proliferating monocyte/macrophage and T-lymphocyte population of cells within the granuloma interacts with and stimulates fibroblasts and other cell activators, with accompanying tissue fibrosis.
In addition, noted in granuloma formation, such as that seen in sarcoid, is the production of calcitriol, lysozyme, and serum ACE. This latter enzyme, generally present in persons younger than 20 years, is normally produced by the endothelial cells of blood vessels. However, in granulomatous disorders, sarcoid in particular, it is more than likely that epithelioid and giant cells actively synthesize ACE. Although present in other granulomatous disorders, a high level of ACE significantly increases the possibility of sarcoid and may be useful in distinguishing sarcoid from other granulomatous disorders. Levels of serum ACE reflect the stage of sarcoid; roughly 67 percent of patients with stage I (bilateral hilar adenopathy) have elevated serum ACE activity, and 95 percent of patients with stage III disease (parenchymal infiltrates of the lung) have the elevated enzyme. With ACE levels of less than 25 U/L, the likelihood ratio for sarcoidosis is 0.12. When the ACE level is between 25 and 71 U/L, the likelihood ratio is 1.31; and when the ACE level is greater than 71 U/L, the likelihood ratio increases to 7.15 (38).
A high probability of sarcoidosis exists in a patient who has arthritis, hilar adenopathy, elevated serum ACE, and a negative purified protein derivative (PPD).
The hypercalcemia and hypercalciuria seen in sarcoidosis are now felt to be the result of increased circulating 1,25-dihydroxyvitamin D. 1,25-Dihydroxyvitamin D has been produced by culturing alveolar macrophages from patients with sarcoidosis. The production of the hormone by the granulomatous tissue itself is more than likely responsible for the abnormal calcium metabolism. Thus, the abnormal increase in 1,25-dihydroxyvitamin D is more than likely from nonrenal sources, as mentioned. The abnormal calcium metabolism results because the nonrenal synthesis of 1,25-dihydroxyvitamin D is not subjected to normal regulatory physiologic mechanisms.
Only gold members can continue reading. Log In or Register to continue