 |
| Figure 8.2 |
External features
Superior view
Anteriorly the frontal bone articulates with the pair of parietal bones at the coronal suture, which runs transversely. The original two halves of the developing frontal bone occasionally fail to fuse, leaving a midline metopic suture. The midline meeting place of the frontal and parietal bones is the bregma, the site of the anterior fontanelle (see Fig. 1.28, p. 32). Behind the bregma the parietal bones articulate in the midline sagittal suture. On either side of the posterior part of this suture a foramen often perforates each parietal bone, through which an emissary vein connects the superior sagittal sinus with scalp veins. The sagittal suture curves down to the lambda, at the apex of the occipital bone.
Posterior view
The lambda is the midline point where the sagittal suture meets the tortuous lambdoid suture between the squamous part of the occipital and the parietal bones (see Fig. 6.84, p. 431). Along these sutures small sutural (Wormian) bones are commonly found.
Some 6 cm below the lambda the occipital bone is projected into the external occipital protuberance, from which a ridge curves, convex upwards, towards the base of the mastoid process. This is the superior nuchal line (Fig. 8.3); gently convex upwards it lies at the junction of neck and scalp. It is the surface marking of the attachment of the tentorium cerebelli and the transverse sinus. Trapezius (medial third) and sternocleidomastoid (lateral half) are attached along the superior nuchal line. Splenius capitis is inserted into the lateral third of the line deep to sternocleidomastoid. Above this a faint, often imperceptible, highest nuchal line gives origin to occipitalis and the galea aponeurotica. Below the superior nuchal line the bone covers the cerebellar hemispheres and gives attachment to muscles at the back of the neck (see p. 430).
The mastoid region of the temporal bone articulates with the parietal and occipital bones, and the mastoid process projects down at the side. The suture between the mastoid and occipital bones is commonly perforated by a mastoid emissary foramen, for a vein which connects the sigmoid sinus with the posterior auricular vein.
Lateral view
To the lateral surface of the mastoid process is attached the sternocleidomastoid, with splenius and longissimus capitis lying deep to it. In front of this is the external acoustic meatus. Above the meatus is a horizontal ridge, the supramastoid crest.
Above the crest the squamous part of the temporal bone extends up to articulate with the parietal bone. The curved anterior border of the squamous part continues to articulate with the parietal bone by its upper part while the lower part articulates with the greater wing of the sphenoid bone. The coronal suture comes down along the side of the skull to reach the curved upper border of the greater wing of the sphenoid, which thus articulates posteriorly with the parietal bone and anteriorly with the frontal bone. The resulting H-shaped pattern of sutures in this region between frontal, parietal, temporal and sphenoid bones is termed the pterion (Fig. 8.1).
The supramastoid crest is projected forwards as the upper border of the zygomatic process of the temporal bone. The zygomatic arch is continued by the zygomatic bone. The frontal process of the zygomatic bone reaches up to meet the frontal bone at the frontozygomatic suture which is palpable in the living. The zygomatic bone has a sharp posterior border which continues up across the suture as a ridge on the frontal bone (Fig. 8.1). This ridge arches up and back and diverges into the superior and inferior temporal lines. The superior line fades posteriorly; the temporalis fascia is attached to it. The inferior temporal line curves down across the squamous temporal bone and turns forwards to join the supramastoid crest.
The temporal fossa is the area bounded by the superior temporal line, zygomatic arch and the frontal process of the zygomatic bone. The temporal fascia is attached above to the superior temporal line and below to the zygomatic arch. Temporalis arises from the inferior temporal line and the whole surface of the temporal fossa below it. The fossa is walled off anteriorly by the concave surface of the zygomatic bone which is here perforated by the zygomaticotemporal nerve.
The zygomatic arch is formed by the zygomatic process of the temporal bone and the temporal process of the zygomatic bone, which meet at an oblique suture near the front end of the arch. (The term ‘zygoma’ is best avoided; it means the arch, though it is often incorrectly used as a name for the zygomatic bone.) The masseter arises mainly from the lower border of the arch, while its posterior deep fibres arise from the medial surface of the arch. The parotidomasseteric fascia is also attached to the lower border of the arch. The arch is crossed in front of the external acoustic meatus by the auriculotemporal nerve and the superficial temporal vessels. Further forward the arch is crossed by the temporal and zygomatic branches of the facial nerve.
The posterior part of the zygomatic process of the temporal bone is described as having anterior and posterior roots. The latter is the backward extension of the arch above the external auditory meatus, its upper border continuing into the supramastoid crest. The anterior root runs medially across the front of the mandibular fossa forming the articular eminence, which is part of the superior articular surface of the temporomandibular joint. Where the anterior root joins the zygomatic arch, the latter has a triangular projection pointing downwards. This is the articular tubercle to which the lateral ligament of the joint is attached.
The zygomatic bone forms the bony prominence of the cheek; it is perforated by the zygomaticofacial foramen for the zygomaticofacial nerve. Zygomaticus major arises from the surface of the zygomatic bone, and zygomaticus minor from the zygomaticomaxillary suture.
The posterior convexity of the maxilla curves backwards towards the lateral pterygoid plate, from which it is separated by the pterygomaxillary fissure. This is closed inferiorly by the pyramidal process (tubercle) of the palatine bone which is wedged between them (see Fig. 6.13, p. 352). The pterygopalatine fossa lies deep to the fissure.
The tuberosity of the maxilla is a bony prominence above the posterior surface of the last molar tooth. The buccinator arises from a linear strip on the maxilla, running forwards from here above the molar teeth. From the tuberosity a fibrous band, the pterygomaxillary ligament (see Fig. 6.13, p. 352), continues the origin of the buccinator to the tip of the hamulus. Deep to the buccinator is the vestibule of the mouth; superficial to it are the soft tissues of the face. From the tuberosity of the maxilla and the pyramidal process of the palatine bone the small superficial head of the medial pterygoid arises, overlapping the inferior head of the lateral pterygoid, which arises from the whole surface of the lateral pterygoid plate. The posterior convexity of the maxilla above the tuberosity shows two or more foramina for the posterior superior alveolar nerves and vessels.
The zygomatic process of the maxilla articulates with the zygomatic bone and with it forms an anterior pillar for the zygomatic arch. It is palpable through the cheek or the vestibule.
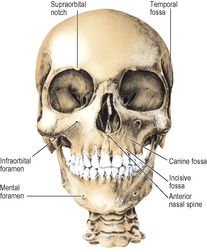
Anterior view
The frontal bone curves down to make the upper margins of the orbits (Fig. 8.2). Medially it goes down to meet the frontal process of each maxilla, between which it articulates with the nasal bones. Laterally it projects down as a zygomatic process to make the frontozygomatic suture with the zygomatic bone at the lateral margin of the orbit. The frontal bone occupies the upper third of the anterior view of the skull, the maxillae and mandible making the other two-thirds.
The nasal bones curve downwards and forwards from their articulation with the frontal bone. Each articulates with the frontal process of the maxilla, and they arch forward to meet in a midline suture. The lower border of each is notched by the external nasal nerve (which also grooves the posterior surface of the nasal bone). These free borders make with the two maxillae a pear-shaped piriform (anterior nasal) aperture (Fig. 8.2). In the nasal cavity the bony septum and the conchae of the lateral wall are visible. The two maxillae meet in a midline intermaxillary suture, and are projected forward as the anterior nasal spine at the lower margin of the nasal aperture. The canine root makes a ridge on the anterior surface of the maxilla, on either side of which are slight depressions, the medial one being the incisive fossa and the lateral the canine fossa, from which levator anguli oris arises and above which the anterior surface of the maxilla is perforated by the infraorbital foramen. Levator labii superioris arises from the lower margin of the orbit above the foramen, from which the infraorbital nerve emerges between these muscles. The line of attachment of buccinator and that of levator anguli oris on the body of the maxilla mark the middle of the maxillary sinus, which lies with its lower half deep to the vestibule and its upper half deep to the soft tissues of the face. The supraorbital notch, infraorbital foramen and mental foramen lie all three in a vertical line, which passes between the two lower premolar teeth. The osteology of the orbital walls and margin is described on page 397.
Inferior view
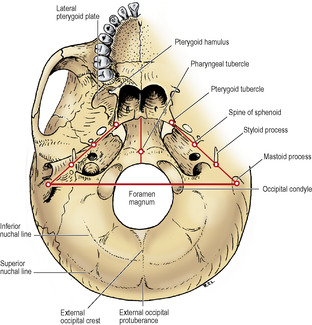
The area behind the foramen magnum consists of the squamous part of the occipital bone. The superior nuchal line lies in a curve concentric with the foramen magnum. Halfway between them the inferior nuchal line is concentric with both. The external occipital crest, in the midline between the external occipital protuberance and the foramen magnum, bisects this area and gives attachment to the ligamentum nuchae. A rather vague line, radiating back and outwards from the foramen magnum, further bisects each half. Thus four areas are demarcated in each half (Fig. 8.3). There are two alongside the foramen magnum to which are attached rectus capitis posterior minor medially, and rectus capitis posterior major laterally (see Fig. 6.84, p. 431). Between superior and inferior nuchal lines semispinalis capitis is attached medially and superior oblique laterally.
One-third of the foramen magnum lies in front and two-thirds behind a line joining the tips of the mastoid processes. The occipital condyles have the reverse proportions; two-thirds of the condyle lies in front of the line.
The foramen magnum is in the basilar part of the occipital bone (basiocciput). The fibrous dura mater is attached to the margins of the foramen as it sweeps down from the posterior cranial fossa. Within the tube of dura mater, the lower medulla with the vertebral and spinal arteries and the spinal roots of the accessory nerves traverse the foramen in the subarachnoid space (see Fig. 6.109, p. 452). Anteriorly the margin of the foramen gives attachment to the ligaments sweeping up from the axis. Adherent to dura mater is the tectorial membrane and in front of this is the vertical limb of the cruciform ligament (see Fig. 6.79, p. 427); in front again are the apical and the pair of alar ligaments of the dens of the axis. Most anteriorly is the attachment of the anterior atlanto-occipital membrane. The posterior atlanto-occipital membrane is attached to the posterior margin of the foramen magnum.
The occipital condyles are convex kidney-shaped surfaces, covered with hyaline cartilage, beside the front half of the foramen magnum. The two convexities make a ball-and-socket joint with the atlas. But the anteroposterior curve is more pronounced than the combined side to side curvature; so the ball is oval-shaped, like an egg lying on its side, and thus permits nodding and some abduction but no rotation. Behind the condyle is the shallow condylar fossa floored by thin bone, commonly perforated by the condylar canal, carrying an emissary vein from the sigmoid sinus to the suboccipital venous plexus. Above the occipital condyle is the hypoglossal canal for the hypoglossal nerve, which emerges medial to the jugular foramen.
The basiocciput extends forward from the foramen magnum and fuses with the basisphenoid. The pharyngeal tubercle is a slight bony prominence in front of the foramen magnum, marking the midline attachment of the pharyngobasilar fascia (see Fig. 6.35, p. 384) and the highest fibres of the superior constrictor. The attachment of the fascia extends on either side of the pharyngeal tubercle along a faint ridge, convex forwards. Behind this is the attachment of the prevertebral fascia, longus capitis and rectus capitis anterior in that order from before backwards immediately in front of the occipital condyle (see Fig. 6.8, p. 345).
The mastoid process is grooved on the deep aspect of its base by the digastric notch for the origin of the posterior belly of the digastric (see Fig. 6.35, p. 384). Medial to this notch a groove for the occipital artery indents the bone along the temporo-occipital suture. The length of the styloid process is very variable. The stylopharyngeus arises high up medially, the stylohyoid high up posteriorly, and the styloglossus low down in front. The stylohyoid ligament passes on from its tip. Between the bases of the styloid and mastoid processes is the stylomastoid foramen, transmitting the facial nerve and the stylomastoid branch of the posterior auricular artery with its accompanying vein. Medial to the styloid process the petrous bone is deeply hollowed out to form the jugular fossa, which with the shallower jugular notch in the occipital bone forms the jugular foramen




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
