27 Orthopaedic surgery
Introduction
Examination
Feel
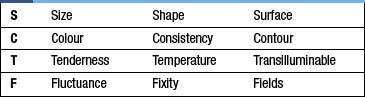
Palpate around the joint or limb. Establish areas of pain, and try to relate these to anatomical structures (e.g. tendons, joint lines etc.). Establish the presence of any swelling and whether this is fluctuant or solid (Table 27.1). Test the neurovascular status of the limb (sensation to light touch and pinprick, and peripheral pulses) and compare with this to the other side.
Investigations
Computed tomography (CT)
CT provides excellent images of bone anatomy (Fig. 27.1) and can be used to supply three-dimensional images to help in the reconstruction of complex fractures. The thin axial slices are particularly useful as a guide for obtaining biopsy specimens

Magnetic resonance imaging (MRI)
MRI (Fig. 27.2) provides excellent images of soft tissue, joint and bone pathology without exposure to radiation. It is widely used in virtually all branches of orthopaedics for diagnosis and preoperative planning.


Description of deformity
With patients in the anatomical position (i.e. lying on their back with their palms pointing up to the ceiling), limb deformities are described relative to the midline (away = valgus, towards = varus) and to the alignment of the limb below the joint or deformity. For example, with respect to the knees, bowleggedness is a varus deformity, while knock-knees are a valgus deformity (Fig. 27.4). With the patient viewed from the side, there is a range of descriptive terms available. For example, hyperextension of the knee joint is known as recurvatum (Fig. 27.5). The three types of spinal deformity are:
• kyphosis: forward flexion (‘the kyphotic kisses his knees’).
• lordosis: the opposite, extension, or bent-over-backwards deformity; this represents the normal alignment of the lumbar and cervical spine.
• scoliosis: a sideward deformity that is normally associated with a degree of rotation (Fig. 27.6).
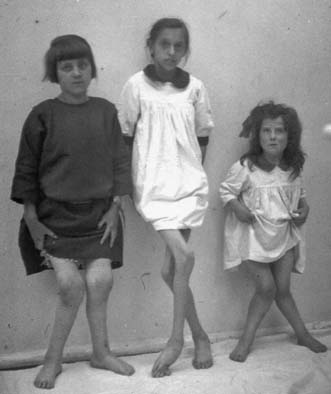
Fig. 27.4 Historical slide of children, showing deformities of the knees.
All the children show valgus knee, i.e. knock-kneed, deformities.


Osteoarthritis: degenerative disease of the joints
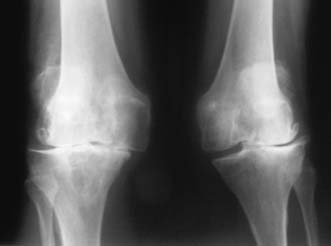
Osteoarthritis (OA) of a joint may occur as a primary idiopathic condition or secondary to problems such as malalignment, intra-articular fractures or over-stressing (obesity, overuse). In some patients, there is a strong genetic component. OA may occur in any joint (shoulder, elbow, wrist and hands) but predominantly affects those that are weight-bearing (hip and knee) (Figs 27.7 and 27.8). Idiopathic OA is generally of slow onset and affects the elderly. Secondary OA can affect the young and may develop quite rapidly when a joint injury leads to loss of articular cartilage. On plain X-ray, OA is associated with:
• joint space loss due to thinning of articular cartilage
• sclerosis of the joint surface, with the development of increased density of the bone just under the joint space


The treatment of OA may be conservative or operative (Table 27.2). The former focuses on the use of drugs and physical methods of pain and stress relief to the joint.
Table 27.2 Management options for osteoarthritis
| Non-operative | Operative |
|---|---|
| Analgesia Physiotherapy Orthotics Injections Lifestyle modifications | Osteotomy Joint debridement Excisional osteotomy Joint replacement (arthroplasty) Joint fusion (arthroplasty) |
Surgical management of OA
Osteotomy
This is useful in the younger patient, in whom joint replacement may not be advisable. The aim is to change the axis of the joint, so that a portion of the joint surface that has thus far been protected from wear and tear now forms the weight-bearing area. For example, with respect to the knee, although there may be severe OA of the medial compartment in conjunction with a varus deformity, the lateral compartment may have well-preserved articular cartilage. Over-correcting the varus deformity by means of osteotomy (removing wedges of bone from the tibia), so that body weight is now largely transmitted through the lateral compartment, may lead to significant improvement in symptoms, thus delaying the need for joint replacement (Fig. 27.9). Osteotomies generally use opening wedges (adding bone), closing wedges (removing bone) or may be translational or rotational.


Joint replacement
Hemi-arthroplasty
In this operation, only one-half of the joint is replaced, leaving half of the joint intact. It is normally the natural socket – for example, the acetabulum – that is left untouched. The most common example is following fracture of the femoral neck in the elderly. Such patients usually have low demand on the joint, and the hemi-arthroplasty (Fig. 27.10) gives adequate function without risking many of the complexities of a total hip replacement.

Total joint replacement
This entails resurfacing of both sides of a joint (Fig. 27.11). The choice of materials for the weight-bearing surfaces varies, depending on the joint and prosthesis in question. Currently, metal against a high-density polyethylene is the most common, although new prostheses involving metal and ceramics surfaces have been developed for use in young people (Fig. 27.12). Fixation of the implants may be with cement, or by encouraging bone to grow into or onto the surface of the implant. In small joints, such as those of the hand in patients with rheumatoid arthritis, silastic may be used as a buffer or spacer between the two joint surfaces.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


