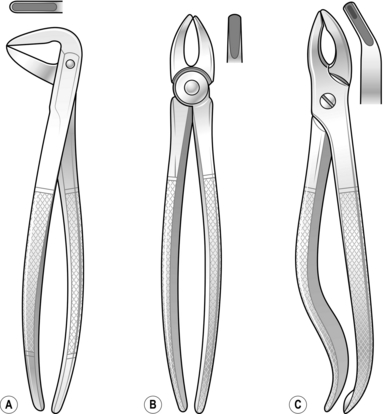
41 1. Most minor procedures such as tooth extraction, biopsy, removal of salivary calculi and suturing of lacerations can be carried out using local analgesia. Local anaesthetics are available in 2-ml glass cartridges, the most common of which contain 2% lidocaine with adrenaline (epinephrine). Use 3% prilocaine with felypressin for patients sensitive to adrenaline (epinephrine). These cartridges fit into a syringe with a disposable needle. 2. In the upper jaw, deposit 1.5 ml of solution over the apex or apices of the offending tooth on the buccal side and about 0.5 ml on the palatal side. In the lower jaw, a similar technique may suffice for the anterior teeth. For the posterior teeth, an inferior alveolar and lingual nerve block is required at the lingula of the mandible, along with a long buccal nerve block at the anterior edge of the ramus of the mandible. Regional nerve block can also be used in the maxilla but, before attempting this, refer to appropriate literature. 3. General anaesthesia is often preferable in the treatment of children, patients who have fluctuant abscesses and if there is a history of allergy to local anaesthetic. 4. Hold the jaws apart with a prop or gag and stabilize the head in a rubber ring or horseshoe. Do not dislocate the jaw or tear the lips, which tend to be dry following preoperative fluid restriction. 5. Lightly coat the lips with petroleum jelly to keep them moist. 1. Remove excess clot. Suture tightly across the socket and repair any lacerations. Apply pressure with a damp gauze pad for 10 minutes, timed by the clock. 2. If bleeding continues, infiltrate local anaesthetic with adrenaline around the area and lightly press a resorbable haemostatic material, such as oxidized cellulose, into the socket. 3. Sit the patient up at least 45° and if necessary give a sedative. 4. Control secondary haemorrhage with pressure, treat infection with systemic antibiotics. A 5-day course of metronidazole and amoxicillin will cover most oral infections. Prescribe 6% hydrogen peroxide mouthwashes. 5. Treat medical causes for prolonged bleeding appropriately, such as haemophilia, thrombocytopenia or hepatic cirrhosis. In patients with haemophilia it is essential to liaise with their haematologist to ensure appropriate factor replacement over the course of the treatment. When dealing with patients on warfarin or antiplatelet medications (e.g. clopidogrel, aspirin) give 5% tranexamic acid as a mouthwash. Flush the socket with the liquid then insert some oxidized cellulose and suture the socket. Prescribe the mouthwash four times a day for 5 days. 6. If the prothrombin time is within the normal therapeutic range, you need not stop the warfarin in order to remove only a few teeth. 1. Use a half-circle 22–24-mm needle with a reverse cutting edge. 2. Use 3/0 sutures. Silk is easy to use but must be removed. Nylon is uncomfortable and also needs to be removed. Polyglactin 910 remains intact in the mouth for 3–4 weeks and produces minimal reaction but the knots and ends are irritating. 3. Use a needle-holder with a ratchet to avoid dropping the needle into the pharynx. 4. Insert the needle into the mucosa 3–5 mm from the edge, taking greater care on the more friable lingual edge. 5. The mucosal edges can rarely be approximated over a socket without excessive removal of bone. If you wish to apply even tension, insert mattress sutures. 6. Tie knots with the needle-holder rather than fingers: this is easier if you keep the end of the suture material short. 1. Warn the patient that, until healing is complete, there may be constant discomfort because of the need to eat, swallow and speak. 2. If necessary, prescribe moderate analgesics such as ibuprofen or paracetamol. Aspirin mixture, used as a gargle, relieves a sore throat caused by an endotracheal tube and packing and ensures more comfortable swallowing. Ice packs applied to the skin for the first 4–6 hours reduce the swelling and subsequent discomfort. 3. Advise the patient that there may be difficulty in opening the mouth wide and chewing may be painful so that a soft diet may be beneficial. 4. Patients who have had their fractured jaws fixed together require special care in the early postoperative hours to avoid inhaling vomit. Swallowed blood may cause vomiting. To avoid this ensure that the stomach is empty preoperatively and administer an anti-emetic. Keep a suction machine and wire-cutters by the bedside and show the nurses which wires to cut in an emergency. 5. When carrying out an operation on bone, many surgeons prescribe prophylactic antibiotics. 1. Is the extraction urgent or will antibiotics give relief until a specialist is available? 2. Tooth removal is indicated when there is a large cavity in a painful tooth, a painful loose tooth resulting from periodontal infection, an alveolar abscess or a loose tooth following trauma that could be inhaled. 1. Extraction forceps: there are three basic pairs (Fig. 41.1), although many more specialized forceps are available. 2. Elevators (levers) enable you to remove broken roots or to loosen teeth before using forceps. 3. Prepare yourself by obtaining a radiograph before tooth removal to display unfavourable curved root patterns, buried roots, impacted teeth and latent pathology. 4. As a rule, have the patient seated, although the supine position is sometimes appropriate. Use local or general anaesthesia. 1. Stand in front of the patient for most extractions. If you are right-handed, it is most convenient to stand behind the patient’s right shoulder to remove lower right teeth. 2. Position the forceps blades on the buccal and lingual aspects of the tooth and push them under the gum as far as they will go along the root. 3. Grip the tooth and move it to expand the socket. 4. Deliver the tooth in the direction of the weakest wall – generally the buccal. 5. Squeeze the socket with your fingers to reduce the dead space and position a damp gauze pad for the patient to bite on until the clot has formed. 6. Instruct the patient to avoid touching the clot for 24 hours and then bathe the wound frequently with warm saline mouth washes until it heals. 7. Leave small broken roots but attempt to remove large superficial roots using fine forceps or elevators. 8. If possible, refer patients with unerupted or impacted teeth to a specialist. Extraction may necessitate removing sufficient bone to allow elevation of the tooth. Use a small chisel or drill to remove the bone. 1. Inspect the socket if infection and pain develop a few days following extraction. 2. If the blood clot has disappeared, the empty socket fills with debris and pus. 3. Syringe out the socket and insert an antiseptic, which usually cures the osteitis. Although the socket closes slowly, a protective epithelial layer soon covers it. 1. Once pus has escaped from bone, its direction of spread is influenced by gravity and muscle attachments. 2. Antibiotics given before there is significant fluctuation may suppress it. 1. If there is no swelling, remove the tooth. Antibiotics are rarely required. 2. Treat a non-fluctuant swelling with antibiotics. The bacteria may be anaerobic. 3. Remove the source of infection if you can provide adequate anaesthesia. 4. When the tooth is partly erupted, clean the underside of the gum flap with an antiseptic solution or 6% hydrogen peroxide. 5. A sharp upper wisdom tooth may traumatize the cheek or the gum over a lower tooth. Removal of the upper is usually simple and gives relief of pain until the more complex lower can be extracted. 6. When fluctuation is present in the mouth, remove the offending tooth if accessible and incise the swelling in the buccal sulcus or palate to release pus that has not emptied into the socket. 7. Pus around the muscles of mastication produces trismus and prevents easy access to posterior teeth. This usually presents as a submandibular abscess. Under general anaesthesia, incise the skin of the neck at the most dependent point of the swelling and parallel to the lower border of the mandible. Extend the wound by blunt dissection then open up the loculi. Pass a pair of sinus forceps to the full depth of the cavity. Open the jaws of the forceps and remove them to enlarge the opening. Repeat this manoeuvre in a plane at right-angles to the original. In large cavities, the septae can be broken down with a finger. 8. Insert a drain for 24–48 hours. If the abscess is extensive, pass the drain from the skin through the abscess cavity and lingual mucosa into the mouth lateral to the submandibular duct. Draw it out of the mouth and fix it to the other end of the drain. 9. Remove the diseased tooth if possible during the anaesthetic period.
Oral and maxillofacial surgery
GENERAL PRINCIPLES OF ORAL SURGERY
Anaesthesia
Haemostasis
Suturing
Aftercare
TOOTH EXTRACTION
Appraise
Prepare
Action
Aftercare
JAW INFECTIONS
DENTAL ABSCESS
Action
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oral and maxillofacial surgery