(1)
Department of Pathology, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
Keywords
JawNeoplasmsOdontogenic tumors4.1 Introduction
Mesenchymal odontogenic tumors are derived from the mesenchymal part of the tissues that participate in development of teeth and periodontal tissues, tooth pulp, dentin, root cementum, periodontal ligament and parts of the bony socket that houses the roots of the teeth. Odontogenic epithelial rests may be part of the histologic picture they show, but represent structures only fortuitously engulfed by tumor tissue. They have no neoplastic or inductive potential.
4.2 Odontogenic Myxoma
Odontogenic myxoma is one of the more common odontogenic tumors [1] and usually occurs in the second or third decade of life. Radiographically, this lesion shows a unilocular or soap bubble appearance (Fig. 4.1). They may occur both in the maxilla as well as in the mandible and involve both anterior and more posterior parts of the jaws (Figs. 4.2 and 4.3). In maxillary cases, the presenting sign may be nasal obstruction due to tumor growth in nasal and paranasal cavities.



Fig. 4.1
Radiograph of mandibular myxoma showing multilocular radiolucency in left mandible
Fig. 4.2
Gross specimen of myxoma. Cut surface shows gelatinous tumor connected with some teeth
Fig. 4.3
Gross specimen of mandibular myxoma. In this case, the tumor shows a more expansive growth causing tooth displacement
The tumor has an extremely gelatinous character that makes it difficult to cut up and take samples for histology; by microscopy, myxomas consist of rather monotonous cells with multipolar or bipolar slender cytoplasmic extensions that lie in a myxoid stroma. Nuclei vary from round to fusiform in appearance, and binucleated cells and mitotic figures may be present but scarce (Figs. 4.4 and 4.5). Adjacent cancellous jaw bone can be engulfed by tumor tissue as there is no demarcation (Figs. 4.6 and 4.7). Cortical perforation and soft tissue extension however do not occur. In this way, the growth pattern of myxoma is identical to that shown by ameloblastoma (Fig. 4.8). Occasionally, the lesion contains odontogenic epithelial rests; they however are a fortuitous finding without any diagnostic or prognostic significance (Fig. 4.9).
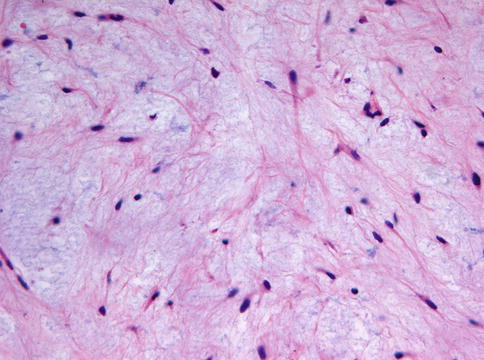
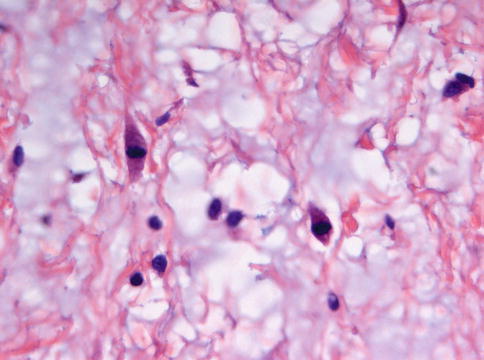
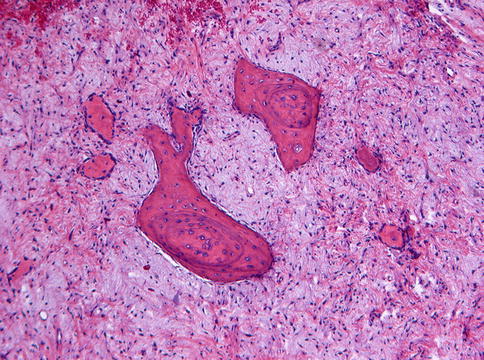
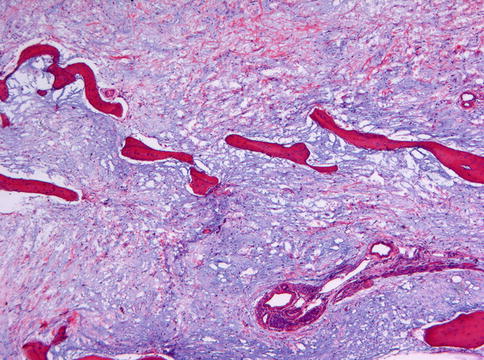
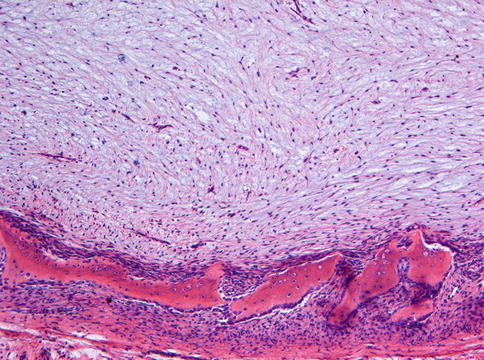
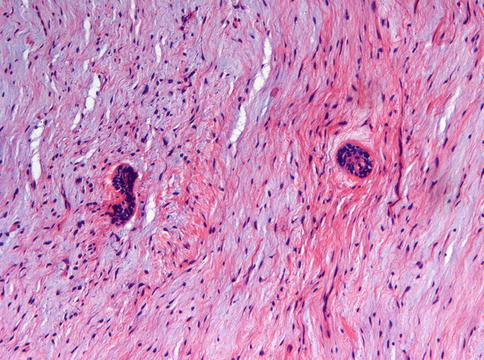
Fig. 4.4
Low power view of myxoma showing cell-poor myxoid tumor tissue
Fig. 4.5
At higher magnification, slight cellular atypia as well as an occasional mitotic figure may be seen
Fig. 4.6
Myxoma. Low power view to show entrapment of adjacent jaw bone by invading tumor tissue
Fig. 4.7
Myxoma invades cancellous bone
Fig. 4.8
Myxoma does not show cortical perforation and spread into adjacent soft tissues. The bordering cortex may only show expansion and attenuation
Fig. 4.9
Odontogenic epithelial nests may occasionally be encountered in myxoma. They are fortuitously engulfed remnants of tooth development and do not have any significance in terms of diagnosis or clinical course
Myxoma cells are positive for vimentin and muscle specific actin, whereas positivity for S-100 is controversial [2–4]. However, immunohistochemistry is of little value in differentiating myxoma from other tumors with a myxoid appearance.
Myxomatous tissue similar as seen in myxoma may also occur in the mixed odontogenic tumors to be discussed in the next Chapter. However, these lesions show abundant epithelial proliferation and occasional deposition of dental hard tissues typically at the interface between epithelial and myxoid tissue components, features not seen in myxoma. Furthermore, myxoma may be mimicked by dental follicle and dental papilla as both may contain myxoid areas [5–8]. Dental papilla tissue can be distinguished from myxoma by the presence of a peripheral layer of columnar odontoblasts and the occasional presence of small fragments of enamel epithelium lying at the periphery of the myxoid tissue, similar as occurs in the tooth germ (Fig. 4.10) or by small fragments of dentin, indicating that the myxoid tissue has focally differentiated into odontoblasts (Fig. 4.11). For both dental papilla and dental follicle clinical and radiographic data are decisive in avoiding misinterpretation of myxomatous tissue in jaw specimens: in the first case, a tooth germ lies in the jaw area from which the submitted tissue has been taken whereas in the second case, the tissue sample covered the crown area of an impacted tooth. The problems how to differentiate between components of the developing teeth and the neoplastic myxoma do not play a role when the formation of the dentition is completed, usually after the 18th year of life. Only in cases occurring at younger age, they are a matter of concern.
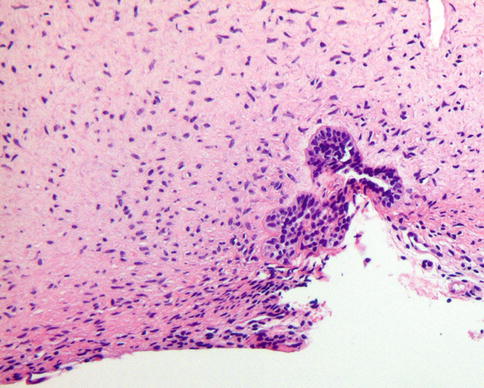
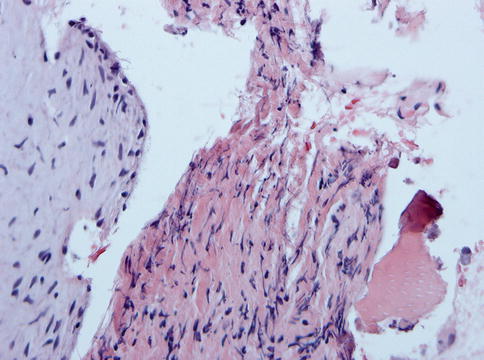
Fig. 4.10
Immature dental papilla tissue may mimic myxoma but can be distinguished by the presence of adjacent columnar enamel epithelium
Fig. 4.11
Presence of dentin also serves to distinguish immature dental papilla from myxoma
Myxoid areas may also occur in neurofibroma and schwannoma. These lesions however are not encountered within the maxillofacial bones.
As the lesion is not encapsulated, treatment should include excision of a margin of uninvolved tissue [9].
4.3 Odontogenic Fibroma
Odontogenic fibroma is a rare lesion; its place within the group of lesions related with tooth development has not yet been firmly established and its differentiation from other jaw lesions that are mainly composed of fibrous tissue is difficult as there is still no agreement about the histologic spectrum these lesions may show [10]. With these caveats in mind, some notes can be made.
Central odontogenic fibromas may present as local bony expansions of the involved jaw area. Quite often, they are incidental findings on radiographs performed for other diagnostic purposes: demarcated unilocular radiolucencies located adjacent to the roots of the neighboring teeth or surrounding impacted tooth (Fig. 4.12) [11].

Fig. 4.12
Radiograph of odontogenic fibroma presenting itself as a radiolucent tumor between the maxillary teeth
As the name already implies, odontogenic fibromas mainly consist of fibroblasts lying in a background of myxoid material intermingled with collagen fibers that may vary from delicate to coarse (Fig. 4.13). Odontogenic epithelium, either scarce or abundant may occur (Figs. 4.14 and 4.15). More variation in histology may occur in cases with extensive cell-rich myxoid areas, a greater epithelial component and varying amounts of amorphous calcified globules or mineralized collagenous matrix. Tumors with this more variegated histology have been referred to as complex odontogenic fibroma or WHO type odontogenic fibroma [10]. Occasionally, odontogenic fibroma may also contain granular cells: such lesions have been called granular cell odontogenic fibroma or, alternatively, granular cell ameloblastic fibroma. This tumor, however, could also represent a unique entity: central odontogenic granular cell tumor [12, 13]. Rarely, this tumor may show atypical histologic features including mitotic activity and aggressive behavior [14].
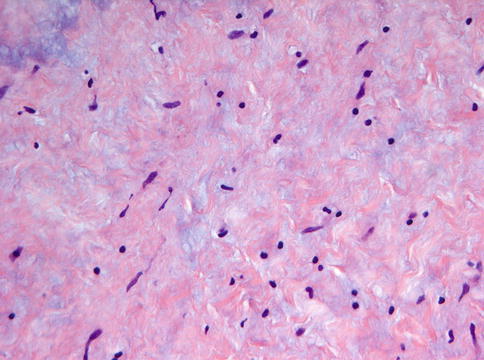
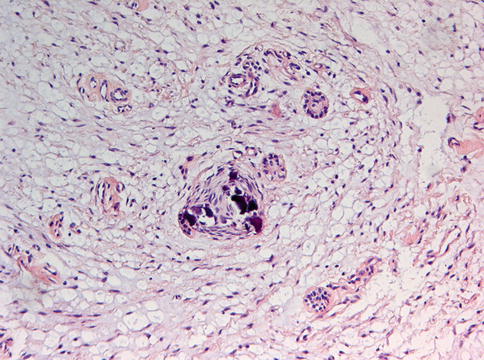
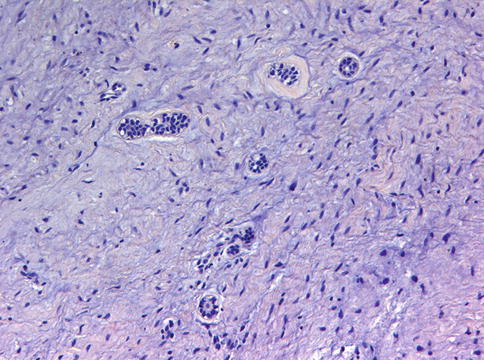
Fig. 4.13
Microscopically, odontogenic fibroma may show the appearance of merely a lump of fibrous tissue without any specific feature. In those cases, the vicinity to a tooth is diagnostic
Fig. 4.14
Occasionally, odontogenic fibroma may show more variation in histology: myxoid areas, calcified material, and odontogenic epithelial rests
Fig. 4.15
Odontogenic epithelial rests by itself are not diagnostic for odontogenic fibroma as they can be found in almost any other jaw lesion
Also, lesions combining histologic features of giant cell granuloma and central odontogenic fibroma have been reported [15–17] and their aggressive nature suggests that the giant cell granuloma component [giant cell granuloma to be discussed in Chap. 8] determines the clinical behavior.
When odontogenic fibromas show a preponderance of myxoid material, distinguishing them from odontogenic myxoma may become problematic. It is probably best to consider such cases to be myxomas and to treat them accordingly. Rarely the epithelial component in odontogenic fibroma may be so conspicuous that its differentiation from ameloblastoma may be difficult [18].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


