Obstructive Nephropathy
Sanjay Jain, MD, PhD
Helen Liapis, MD
Key Facts
Terminology
Acute or chronic damage to kidney due to obstruction of urine flow
Etiology/Pathogenesis
Many causes, congenital and acquired
Developmental defect
Neoplasia
Stones
UPJO most common cause
Clinical Issues
Chronic or repeated pyelonephritis
Flank pain
Hypertension
Renal failure (bilateral)
Macroscopic Features
Dilatation of pelvis (hydronephrosis), blunting of calyces
Marked loss of medulla, cortical thinning
Microscopic Pathology
Marked loss of tubules
Global and segmental glomerulosclerosis
Interstitial fibrosis, chronic inflammation
Dilation of collecting ducts
Dysplasia indicates congenital origin
Top Differential Diagnoses
Reflux nephropathy
Tubulointerstitial diseases
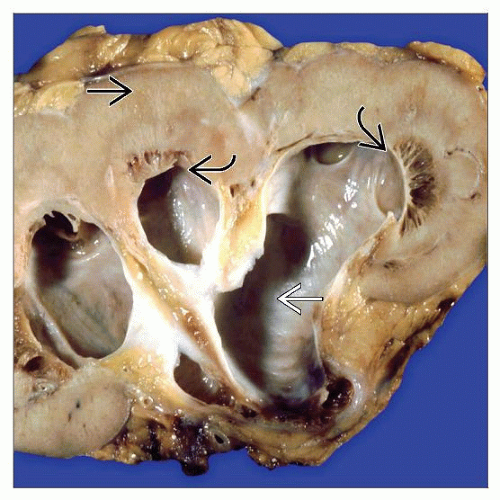 The typical features of chronic obstruction include dilation of the pelvis and calyces (hydronephrosis)  , loss of the medullary pyramids , loss of the medullary pyramids  , and secondary thinning of the cortex , and secondary thinning of the cortex  . . |
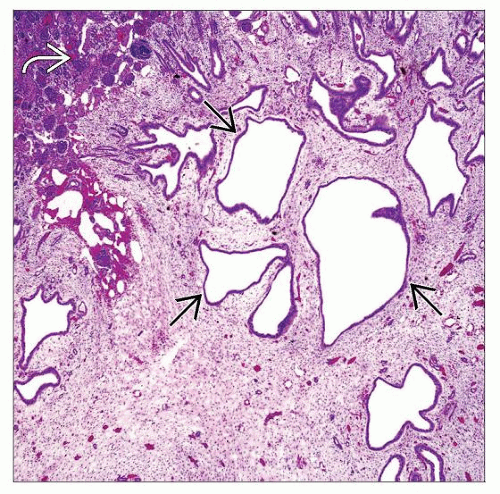 A section of the medulla from a child with UPJO shows dilation of the larger medullary collecting ducts  due to increased urine back-pressure. The cortex is relatively spared due to increased urine back-pressure. The cortex is relatively spared  . . |
TERMINOLOGY
Definitions
Obstructive nephropathy
Damage to kidney due to urine flow obstruction
Hydronephrosis
Dilatation of renal pelvis due to functional or physical impediment to urine flow
ETIOLOGY/PATHOGENESIS
Causes
Physical obstruction
Stone
Tumors of the urinary tract
Prostate, bladder, ureter
Benign prostate hyperplasia (BPH)
External compression (tumors, pregnancy, retroperitoneal fibrosis, endometriosis, crossing vessels)
Functional obstruction
Developmental anomalies: Posterior urethral valves (PUV), ureterocele, ureteropelvic junction obstruction (UPJO), primary megaureter
UPJO is most common cause of obstructive nephropathy
Pathophysiology
Impediment to urine flow causes increase in back-pressure into collecting system and tubules
Increased back-pressure and retention of urine causes dilatation of collecting system and alterations in transporters and channels
Compression of renal parenchyma accompanies vascular compromise and inflammatory response
Cellular changes in interstitium and nephrons lead to varying degrees of scarring
Intrauterine obstruction during nephrogenesis can cause renal dysplasia
Animal Models
Unilateral ureteral obstruction (UUO)
Commonly used in rodents, marsupials
Genetic models
Provide evidence for functional defects rather than physical causes of obstructive nephropathy (Aqp2 mutations)
CLINICAL ISSUES
Presentation
Acute obstruction
Flank pain, nausea, and vomiting
Renal failure if bilateral
Chronic obstruction
Recurrent episodes of pyelonephritis
Hypertension
Renal failure if bilateral
Treatment
Surgical repair
Decompression
Prognosis
Prognostic criteria for congenital impediments to urine flow are not well defined; therefore, management criteria are debatable
Kidney failure may ensue if accompanied by dysplasia due to congenital obstruction
Correction of congenital obstruction may not resolve kidney damage; children should be followed into adulthood
High propensity to develop renal insufficiency in PUV patients
IMAGE FINDINGS
Ultrasonographic Findings
Dilated pelvis
MACROSCOPIC FEATURES
General Features
Dilatation of pelvis (hydronephrosis), blunting of calyces
Compression of the cortex
Irregular kidney surface due to scarring
Other anomalies or syndromes may be present: Hydronephrosis, small kidneys, duplicated collecting system, megaureter, hydroureter, dysplastic kidneys
Compensatory hypertrophy in contralateral kidney
MICROSCOPIC PATHOLOGY
Histologic Features
Glomeruli
Glomeruli relatively spared but eventually become globally sclerotic
Periglomerular fibrosis prominent
Global glomerulosclerosis, obsolescent glomeruli, glomerular cysts
Atubular glomeruli (cystic dilation of Bowman space)
Crescents seen rarely
Increased glomerular size in contralateral kidney
Tubules
Tubular atrophy, apoptosis
Thyroidization of tubules (end-stage atrophy)
Microcystic dilatation of distal nephron segments
Dilation of tubules may be more prominent in subcapsular collecting ducts
Rupture with leakage of Tamm-Horsfall protein
Interstitium
Fibrosis, diffuse
Mononuclear inflammation, plasma cells
Sometimes intense in sites of tubular rupture
Presence of cartilage or smooth muscle indicative of dysplasia
Segmental (lobar) or zonal (outer cortex) distribution
Vessels
Arterial medial hypertrophy and intimal fibroelastosis are indicative of hypertension
Pelvis and ureter
Pelvic dilatation, papillae effacement
Hypertrophy and dilation of ureter
Chronic inflammation mucosa of pelvis and ureter
Acute Obstruction
May have few pathologic findings
Interstitial edema, mild inflammation
Dilation of subcapsular collecting ducts
Dilated lymphatics contain Tamm-Horsfall protein
DIFFERENTIAL DIAGNOSIS



