Neuroendocrine tumor (NET), G1 (carcinoid) or G2
Neuroendocrine carcinoma (NEC), G3, large cell or small cell type
Mixed adenoneuroendocrine carcinoma (MANEC)
Hyperplastic and preneoplastic lesions
Interlaboratory variability resulting from use of different antibodies and different techniques remains a serious problem. Despite this variability, the predictability and reproducibility of standardized IHC reagents, such as monoclonal antibodies, has made the use of these reagents to characterize neuroendocrine neoplasms widely accepted.
TABLE 11.1 Cells and Neoplasms of the Dispersed Neuroendocrine Systema | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
TABLE 11.2 Sites of Eutopic and Ectopic Hormone Production of Common Neuroendocrine Hormones | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
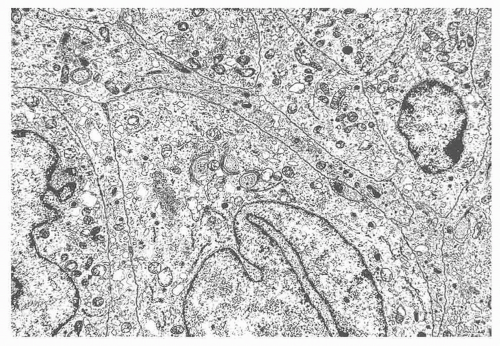 FIGURE 11.1 Neuroendocrine carcinoma of lung from a patient with Cushing syndrome. The carcinoma was positive for adrenocorticotropic hormone and corticotropin-releasing hormone by immunostaining. Neurosecretory granules ranging in size from 100 to 300 nm in diameter are present in the cytoplasm (8600×). |
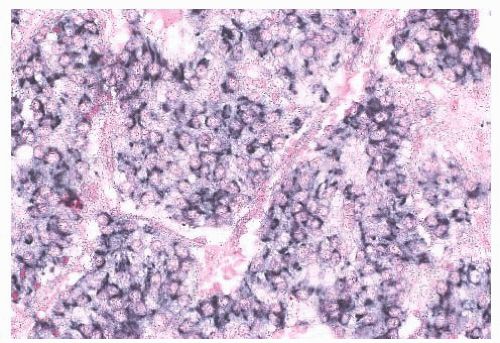 FIGURE 11.2 In situ hybridization localizing chromogranin A RNA diffusely in a retroperitoneal neuroendocrine tumor (in situ hybridization with a digoxigenin-labeled probe cocktail of chromogranin A and B with streptavidin nitroblue tetrazolium-5-bromo-4-chloro-3-indolyl phosphate [NBT-BCIP] detection). |
as chromogranin, immunoreactivity in most tumors. ACTH, somatostatin, calcitonin, and other peptides have also been found (41,42). Because thymic NETs have a broad range of histologic appearances, the differential diagnosis includes many lesions. Epithelial thymomas, germ cell tumors, and lymphomas are non-NETs that should be considered in the differential diagnosis. IHC staining for broad-spectrum neuroendocrine markers, such as chromogranins and synaptophysin, can usually exclude these other tumors. Parathyroid and thyroid neoplasms; paragangliomas; and other metastatic neuroendocrine carcinomas, including poorly differentiated (small cell) neuroendocrine carcinomas, medullary thyroid carcinomas, pulmonary NETs, and pancreatic NETs, should all be part of the differential diagnosis. IHC staining does not differentiate between thymic NETs and other neuroendocrine neoplasms.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


